

A tailored approach in lymph node-positive perihilar cholangiocarcinoma
- PMID: 34075473
- PMCID: PMC8370897
- DOI: 10.1007/s00423-021-02154-4
A tailored approach in lymph node-positive perihilar cholangiocarcinoma
Erratum in
-
Correction to: A tailored approach in lymph node-positive perihilar cholangiocarcinoma.Langenbecks Arch Surg. 2022 Dec;407(8):3903-3905. doi: 10.1007/s00423-021-02332-4. Langenbecks Arch Surg. 2022. PMID: 34718877 Free PMC article. No abstract available.
Abstract
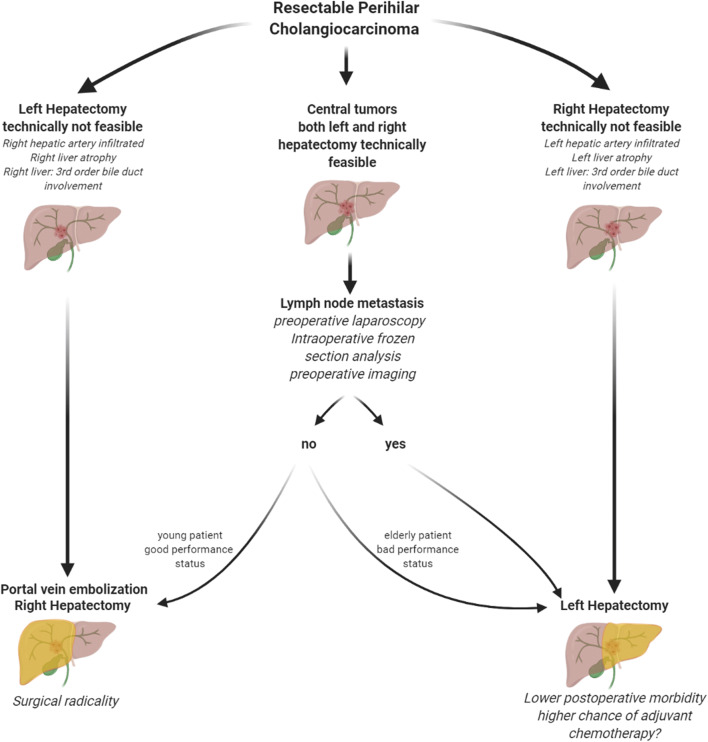
Purpose: Extended right hepatectomy is associated with wide surgical margins in PHC and often favored for oncological considerations. However, it remains uncertain whether established surgical principles also apply to the subgroup of node-positive patients. The aim of the present study was to define a tailored surgical approach for patients with perihilar cholangiocarcinoma (PHC) and lymph node metastases.
Methods: We reviewed the course of all consecutive patients undergoing major hepatectomy for PHC between 2005 and 2015 at the Department of Surgery, Charité - Universitätsmedizin Berlin.
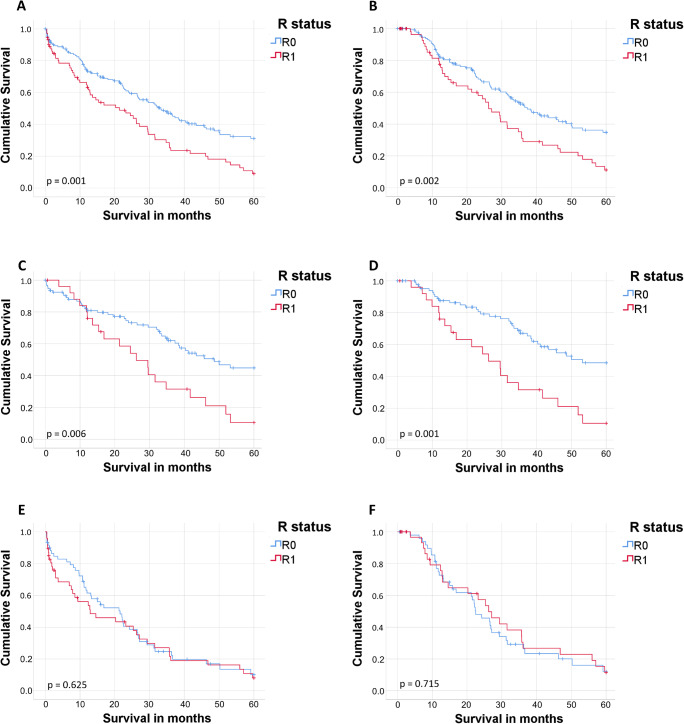
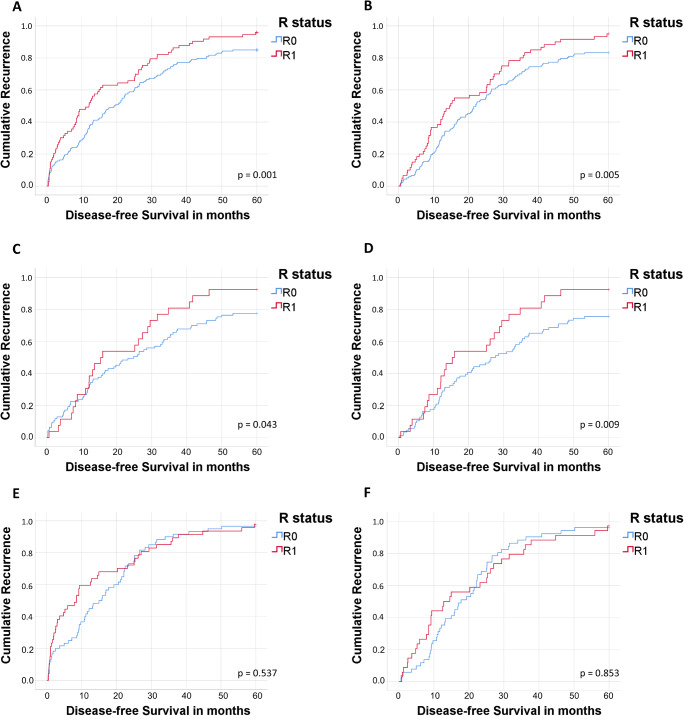
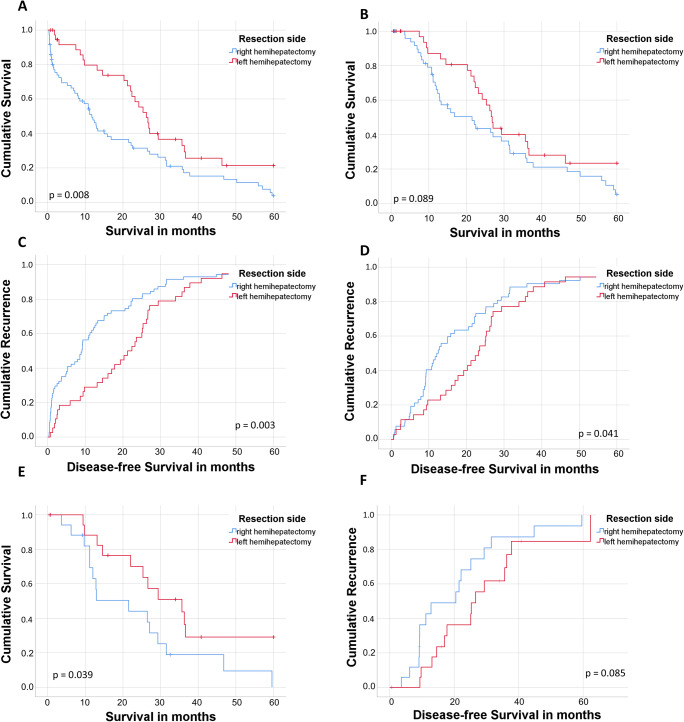
Results: Two hundred and thirty-one patients underwent major hepatectomy for PHC with 1-, 3-, and 5-year overall (OS) and disease-free survival (DFS) rates of 72%, 48%, and 36%, and 60%, 22%, and 12%, respectively. In lymph node-positive patients (n = 109, 47%), extended left hepatectomy was associated with improved OS and DFS, respectively, when compared to extended right hepatectomy (p = 0.008 and p = 0.003). Interestingly, OS and DFS did not differ between R0 and R1 resections in those patients (both p = ns). Patients undergoing extended left hepatectomy were more likely to receive adjuvant chemotherapy (p = 0.022). This is of note as adjuvant chemotherapy, besides grading (p = 0.041), was the only independent prognostic factor in node-positive patients (p=0.002).
Conclusion: Patients with node-positive PHC might benefit from less aggressive approaches being associated with lower morbidity and a higher chance for adjuvant chemotherapy. Lymph node sampling might help to guide patients to the appropriate surgical approach according to their lymph node status.
Keywords: Long-term survival; Lymph node positive perihilar cholangiocarcinoma; Major hepatectomy; Postoperative complications.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
High-grade dysplasia/carcinoma in situ of the bile duct margin in patients with surgically resected node-negative perihilar cholangiocarcinoma is associated with poor survival: a retrospective study.J Hepatobiliary Pancreat Sci. 2017 Aug;24(8):456-465. doi: 10.1002/jhbp.481. Epub 2017 Jul 3. J Hepatobiliary Pancreat Sci. 2017. PMID: 28547855
-
Perihilar cholangiocarcinoma: A different concept for radical resection.Surg Oncol. 2020 Jun;33:270-275. doi: 10.1016/j.suronc.2020.02.013. Epub 2020 Feb 17. Surg Oncol. 2020. PMID: 32561092
-
Left-sided Hepatectomy Leads to Less Postoperative Liver Failure and Comparable Overall Survival to Right-sided Hepatectomy in Type II or IV Perihilar Cholangiocarcinoma.Ann Surg Oncol. 2023 Mar;30(3):1381-1390. doi: 10.1245/s10434-022-12756-x. Epub 2022 Nov 10. Ann Surg Oncol. 2023. PMID: 36357701
-
Textbook outcome after major hepatectomy for perihilar cholangiocarcinoma - definitions and influencing factors.Langenbecks Arch Surg. 2022 Jun;407(4):1561-1573. doi: 10.1007/s00423-022-02467-y. Epub 2022 Mar 4. Langenbecks Arch Surg. 2022. PMID: 35246771 Free PMC article.
-
[Klatskin tumor. A study of 15 resected cases].Chirurgie. 1999 Apr;124(2):132-9; discussion 139-40. doi: 10.1016/s0001-4001(99)80055-5. Chirurgie. 1999. PMID: 10349749 Review. French.
Cited by
-
Impact of Positive Lymph Nodes and Resection Margin Status on the Overall Survival of Patients with Resected Perihilar Cholangiocarcinoma: The ENSCCA Registry.Cancers (Basel). 2022 May 12;14(10):2389. doi: 10.3390/cancers14102389. Cancers (Basel). 2022. PMID: 35625993 Free PMC article.
-
Prediction of regional lymph node metastasis in intrahepatic cholangiocarcinoma: it's not all about size.Abdom Radiol (NY). 2023 Oct;48(10):3063-3071. doi: 10.1007/s00261-023-03991-1. Epub 2023 Jun 24. Abdom Radiol (NY). 2023. PMID: 37354262 Free PMC article.
-
A surgical strategy for intrahepatic cholangiocarcinoma - the hilar first concept.Langenbecks Arch Surg. 2023 Aug 7;408(1):296. doi: 10.1007/s00423-023-03023-y. Langenbecks Arch Surg. 2023. PMID: 37544932 Free PMC article.
-
Parenchyma-Preserving Hepatectomy in Perihilar Cholangiocarcinoma: A Chance for Critical Patients?Visc Med. 2024 Apr;40(2):53-60. doi: 10.1159/000537884. Epub 2024 Mar 22. Visc Med. 2024. PMID: 38584859 Free PMC article.
-
Feasibility and Efficacy of Adjuvant Chemotherapy With Gemcitabine After Liver Transplantation for Perihilar Cholangiocarcinoma - A Multi-Center, Randomized, Controlled Trial (pro-duct001).Front Oncol. 2022 Oct 6;12:910871. doi: 10.3389/fonc.2022.910871. eCollection 2022. Front Oncol. 2022. PMID: 36330499 Free PMC article.
References
-
- Ethun CG, Lopez-Aguiar AG, Anderson DJ, Adams AB, Fields RC, Doyle MB, Chapman WC, Krasnick BA, Weber SM, Mezrich JD, Salem A, Pawlik TM, Poultsides G, Tran TB, Idrees K, Isom CA, Martin RCG, Scoggins CR, Shen P, Mogal HD, Schmidt C, Beal E, Hatzaras I, Shenoy R, Cardona K, Maithel SK. Transplantation versus resection for hilar cholangiocarcinoma: an argument for shifting treatment paradigms for resectable disease. Ann Surg. 2018;267(5):797–805. doi: 10.1097/sla.0000000000002574. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
