

Development and validation of antibiotic stewardship metrics for outpatient respiratory tract diagnoses and association of provider characteristics with inappropriate prescribing
- PMID: 34075872
- PMCID: PMC9904452
- DOI: 10.1017/ice.2021.44
Development and validation of antibiotic stewardship metrics for outpatient respiratory tract diagnoses and association of provider characteristics with inappropriate prescribing
Abstract
Objective: To determine metrics and provider characteristics associated with inappropriate antibiotic prescribing for respiratory tract diagnoses (RTDs).
Design: Retrospective cohort study.
Setting: Primary care practices in a university health system.
Participants: Patients seen by an attending physician or advanced practice provider (APP) at their primary care office visit with International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM)-coded RTDs.
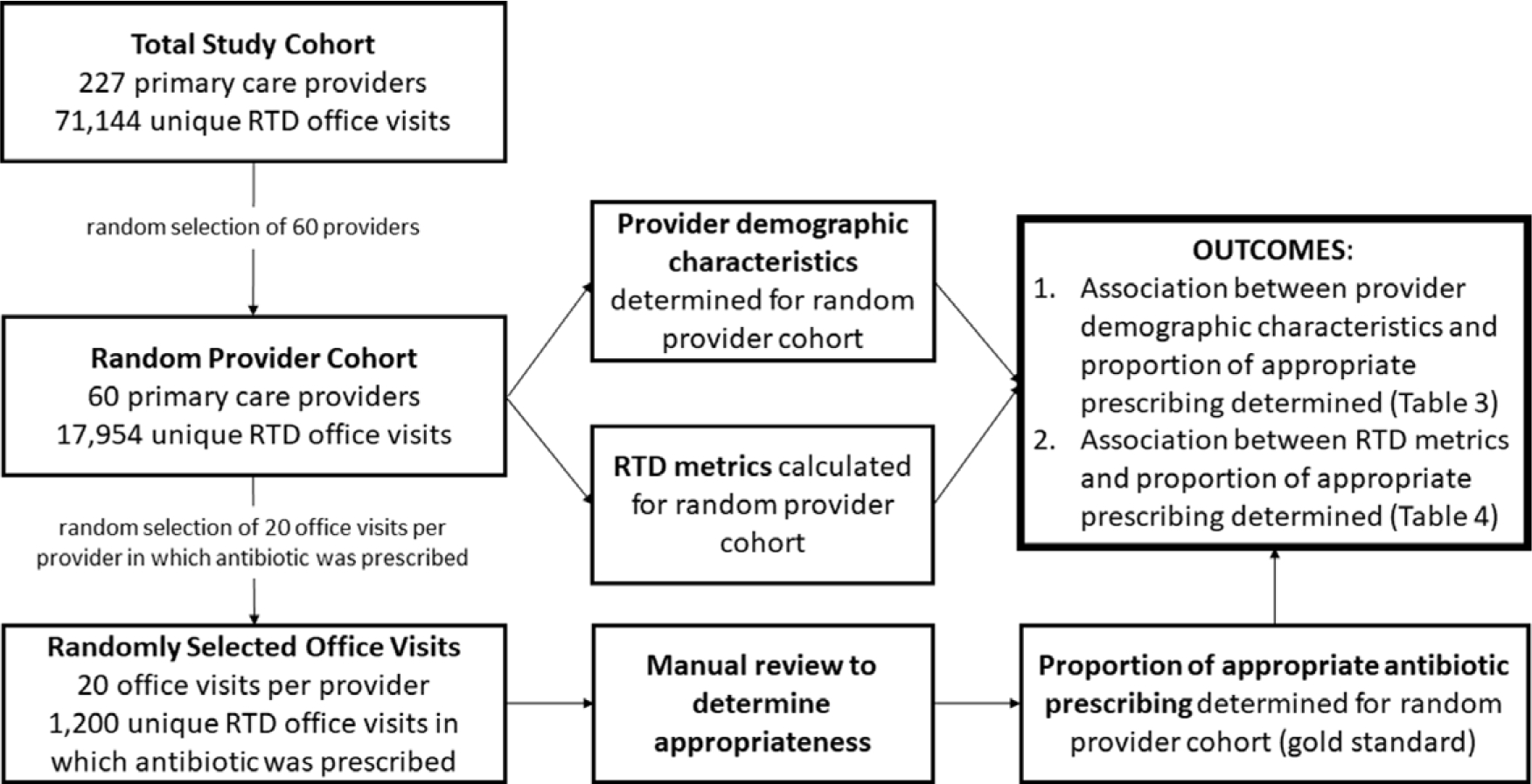
Methods: Medical records were reviewed for 1,200 randomly selected office visits in which an antibiotic was prescribed to determine appropriateness. Based on this gold standard, metrics and provider characteristics associated with inappropriate antibiotic prescribing were determined.
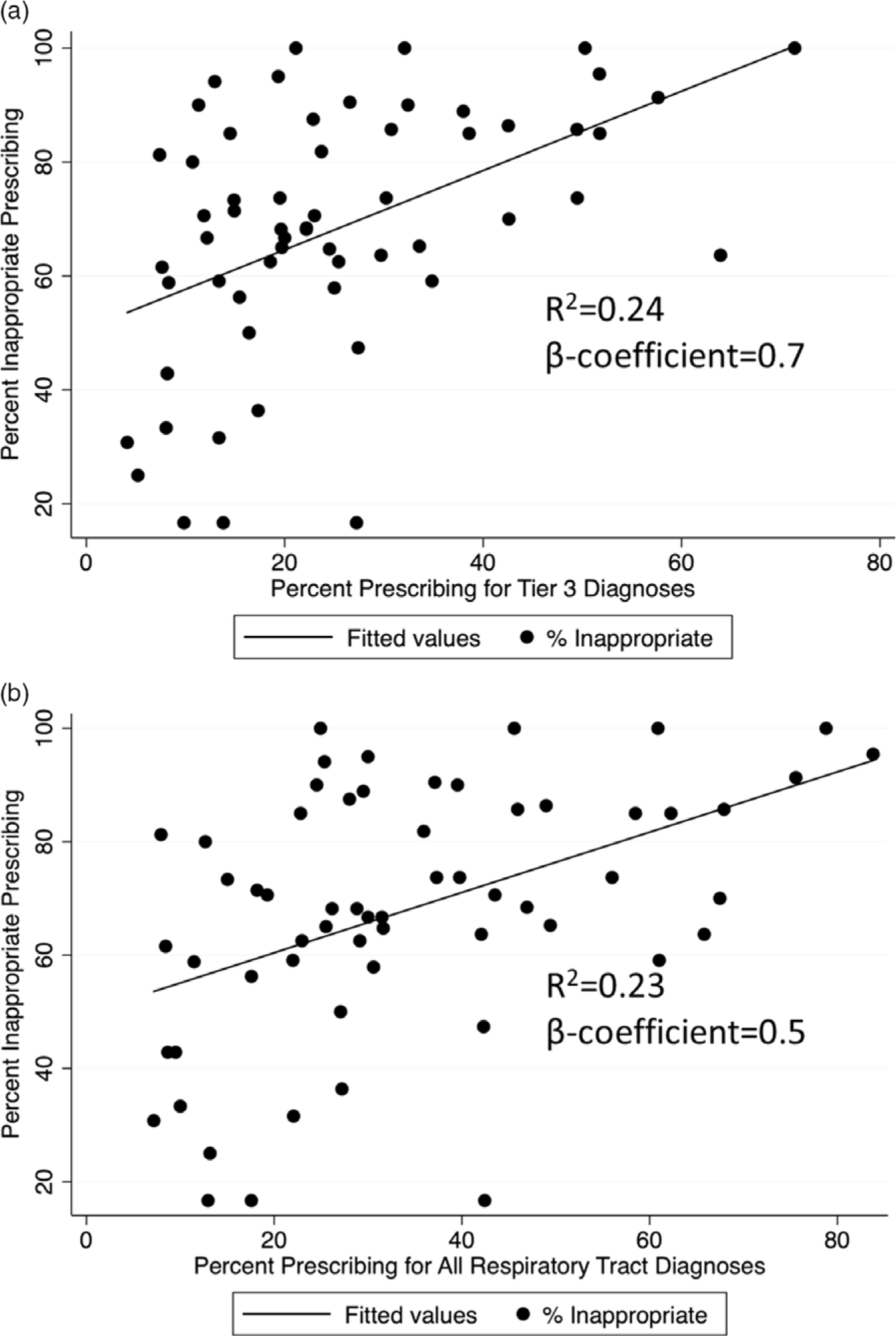
Results: Overall, 69% of antibiotics were inappropriate. Metrics utilizing prespecified RTDs most strongly associated with inappropriate prescribing were (1) proportion prescribing for RTDs for which antibiotics are almost never required (eg, bronchitis) and (2) proportion prescribing for any RTD. Provider characteristics associated with inappropriate antibiotic prescribing were APP versus physician (72% vs 58%; P = .02), family medicine versus internal medicine (76% vs 63%; P = .01), board certification 1997 or later versus board certification before 1997 (75% vs 63%; P = .02), nonteaching versus teaching practice (73% vs 51%; P < .01), and nonurban vs urban practice (77% vs 57%; P < .01).
Conclusions: Metrics utilizing proportion prescribing for RTDs for which antibiotics are almost never required and proportion prescribing for any RTD were most strongly associated with inappropriate prescribing. APPs and clinicians with family medicine training, with board certification 1997 or later, and who worked in nonteaching or nonurban practices had higher proportions of inappropriate prescribing. These findings could inform design of interventions to improve prescribing and could represent an efficient way to track inappropriate prescribing.
Conflict of interest statement
Figures
Similar articles
-
Improving Outpatient Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: A Stepped-Wedge Cluster Randomized Trial.Clin Infect Dis. 2022 Mar 23;74(6):947-956. doi: 10.1093/cid/ciab602. Clin Infect Dis. 2022. PMID: 34212177 Free PMC article. Clinical Trial.
-
Patient, Provider, and Practice Characteristics Associated with Inappropriate Antimicrobial Prescribing in Ambulatory Practices.Infect Control Hosp Epidemiol. 2018 Mar;39(3):307-315. doi: 10.1017/ice.2017.263. Epub 2018 Jan 30. Infect Control Hosp Epidemiol. 2018. PMID: 29378672
-
Analysis of seasonal variation of antibiotic prescribing for respiratory tract diagnoses in primary care practices.Antimicrob Steward Healthc Epidemiol. 2023 Sep 5;3(1):e147. doi: 10.1017/ash.2023.418. eCollection 2023. Antimicrob Steward Healthc Epidemiol. 2023. PMID: 37771744 Free PMC article.
-
Behavioral Economics and Ambulatory Antibiotic Stewardship: A Narrative Review.Clin Ther. 2021 Oct;43(10):1654-1667. doi: 10.1016/j.clinthera.2021.08.004. Epub 2021 Oct 23. Clin Ther. 2021. PMID: 34702589 Free PMC article. Review.
-
Interventions to reduce inappropriate prescribing of antibiotics for acute respiratory tract infections: summary and update of a systematic review.J Int Med Res. 2018 Aug;46(8):3337-3357. doi: 10.1177/0300060518782519. Epub 2018 Jul 1. J Int Med Res. 2018. PMID: 29962311 Free PMC article.
Cited by
-
Improving Outpatient Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: A Stepped-Wedge Cluster Randomized Trial.Clin Infect Dis. 2022 Mar 23;74(6):947-956. doi: 10.1093/cid/ciab602. Clin Infect Dis. 2022. PMID: 34212177 Free PMC article. Clinical Trial.
-
Adaptation and validation of an antibiotic prescribing, peer comparison metric for respiratory tract diagnoses in walk-in clinics: a mixed-methods analysis.Antimicrob Steward Healthc Epidemiol. 2024 Oct 16;4(1):e176. doi: 10.1017/ash.2024.436. eCollection 2024. Antimicrob Steward Healthc Epidemiol. 2024. PMID: 39450095 Free PMC article.
-
Evaluation of appropriateness of antibiotic prescribing in primary healthcare institutions in China using proxy indicator.Lancet Reg Health West Pac. 2024 Jul 2;49:101132. doi: 10.1016/j.lanwpc.2024.101132. eCollection 2024 Aug. Lancet Reg Health West Pac. 2024. PMID: 39056089 Free PMC article.
-
Appropriateness of intended antibiotic prescribing using clinical case vignettes in primary care, and related factors.Eur J Gen Pract. 2024 Dec;30(1):2351811. doi: 10.1080/13814788.2024.2351811. Epub 2024 May 20. Eur J Gen Pract. 2024. PMID: 38766775 Free PMC article.
-
Antibiotic Prescribing Patterns for Respiratory Tract Illnesses Following the Conclusion of an Education and Feedback Intervention in Primary Care.Clin Infect Dis. 2024 May 15;78(5):1120-1127. doi: 10.1093/cid/ciad754. Clin Infect Dis. 2024. PMID: 38271275 Free PMC article.
References
-
- Centers for Disease Control and Prevention. 2019 Antimicrobial resistance threats report. https://www.cdc.gov/drugresistance/biggest-threats.html. Accessed September 24, 2020.
-
- Suda KJ, Hicks LA, Roberts RM, et al. A national evaluation of antibiotic expenditures by healthcare setting in the United States, 2009. J Antimicrob Chemother 2013;68:715–718. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016;315:1864–1873. - PubMed
-
- Gonzales R, Malone DC, Maselli JH, Sande MA. Excessive antibiotic use for acute respiratory infections in the United States. Clin Infect Dis 2001;33:757–762. - PubMed
-
- Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core elements of outpatient antibiotic stewardship. MMWR Recomm Rep 2016;65(RR-6):1–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
