

Low-dose ketamine does not improve the speed of recovery from depression in electroconvulsive therapy: a randomized controlled trial
- PMID: 34076068
- PMCID: PMC8827368
- DOI: 10.1590/1516-4446-2020-1705
Low-dose ketamine does not improve the speed of recovery from depression in electroconvulsive therapy: a randomized controlled trial
Abstract
Objective: Electroconvulsive therapy (ECT) is a well-established therapeutic intervention for major depressive disorder. Recent literature has shown that the anesthetic agent ketamine has some antidepressant properties at low doses and may be an alternative therapy for treatment-resistant major depressive disorder. We hypothesized that the use of low-dose ketamine as an anesthetic adjunct in ECT would more rapidly improve depression while maintaining hemodynamic stability than ECT with propofol alone.
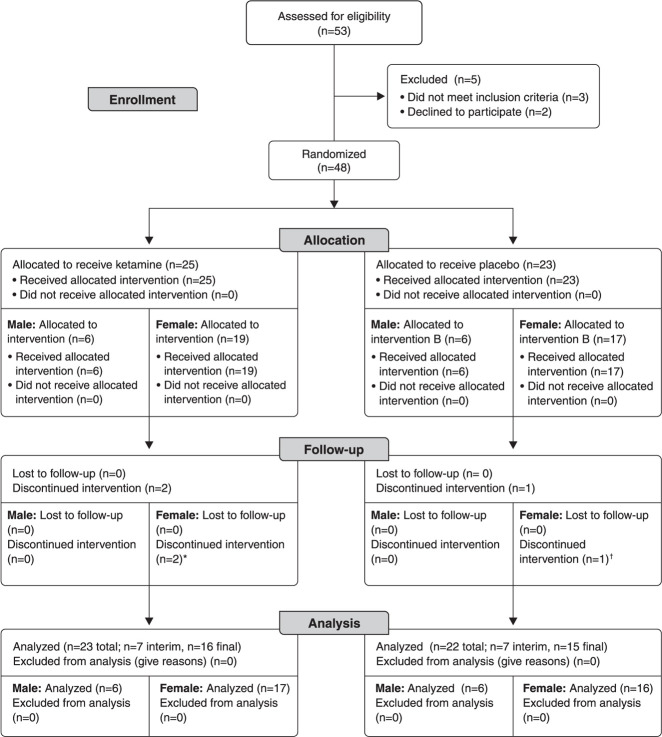
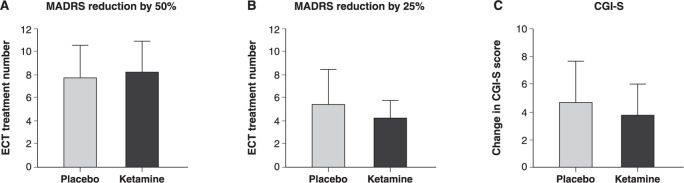
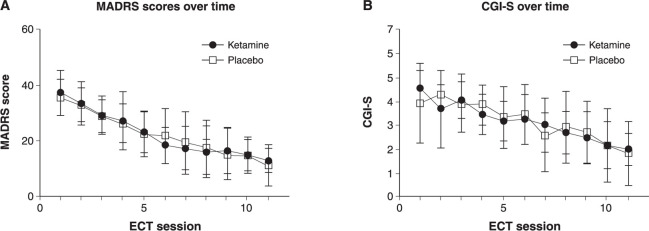
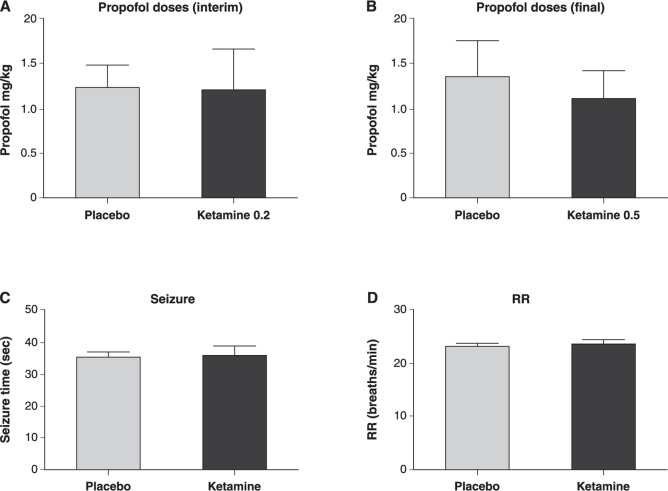
Methods: Institutional ethics approval was obtained, and the use of ketamine in this study was approved by Health Canada. This is a randomized, double-blinded, placebo-controlled trial that involved ketamine administration at 0.5 mg/kg IV in addition to propofol anesthesia for ECT. The primary outcome was the number of ECT treatments required to achieve a 50% reduction in the Montgomery-Asberg Depression Rating Scale (MADRS). Secondary outcomes included the number of ECT treatments required to achieve a 25% reduction in MADRS score, as well as any differences in the Clinical Global Impression Scale for Severity, hemodynamic variables, and seizure duration. Adverse events were recorded for safety assessment.
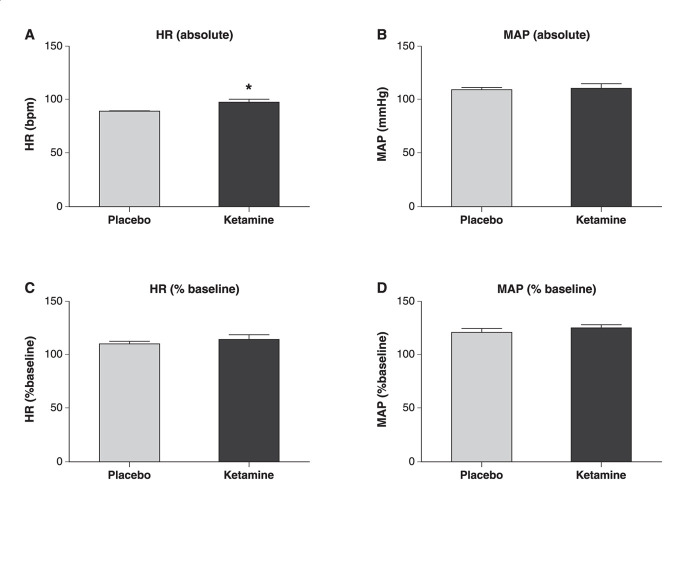
Results: A total of 45 patients completed the study. No difference was found between groups with respect to the primary or secondary outcomes. The ketamine group showed a trend towards a decreased dose of propofol required to achieve adequate anesthesia. No adverse events were reported.
Conclusion: Low-dose ketamine does not improve psychiatric outcomes in the setting of propofol-based anesthesia for ECT. Specifically, ketamine did not reduce the number of ECT sessions necessary to achieve a 50 or 25% reduction in MADRS scores. Reassuringly, the fact that no differences in hemodynamic variables or unexpected adverse events occurred suggests that low-dose ketamine may be safely used in this setting should clinical indications warrant its use.
Clinical trial registration: ClinicalTrials.gov, NCT02579642.
Conflict of interest statement
CM participated in the Regional Canadian Esketamine Advisory Board Meeting (AB-SK-MB, Feb 13 2019), which provided a clinical review of Esketamine, examined evidence for its use, and reviewed safety protocols. The other authors report no conflicts of interest.
Figures
References
-
- Petrides G, Fink M, Husain MM, Knapp RG, Rush AJ, Mueller M, et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: a report from CORE. J ECT. 2001;17:244–53. - PubMed
-
- Takano H, Motohashi N, Uema T, Ogawa K, Ohnishi T, Nishikawa M, et al. Differences in cerebral blood flow between missed and generalized seizures with electroconvulsive therapy: a positron emission tomographic study. Epilepsy Res. 2011;97:225–8. - PubMed
-
- Andrade C, Bolwig TG. Electroconvulsive therapy, hypertensive surge, blood-brain barrier breach, and amnesia: exploring the evidence for a connection. J ECT. 2014;30:160–4. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
