

National variation in the delivery of radiation oncology procedures in the non-facility-based setting
- PMID: 34076341
- PMCID: PMC8290244
- DOI: 10.1002/cam4.4028
National variation in the delivery of radiation oncology procedures in the non-facility-based setting
Abstract
Purpose: Though utilization of medical procedures has been shown to vary considerably across the United States, similar efforts to characterize variation in the delivery of radiation therapy (RT) procedures have not been forthcoming. Our aim was to characterize variation in the delivery of common RT procedures in the Medicare population. We hypothesized that delivery would vary significantly based on provider characteristics.
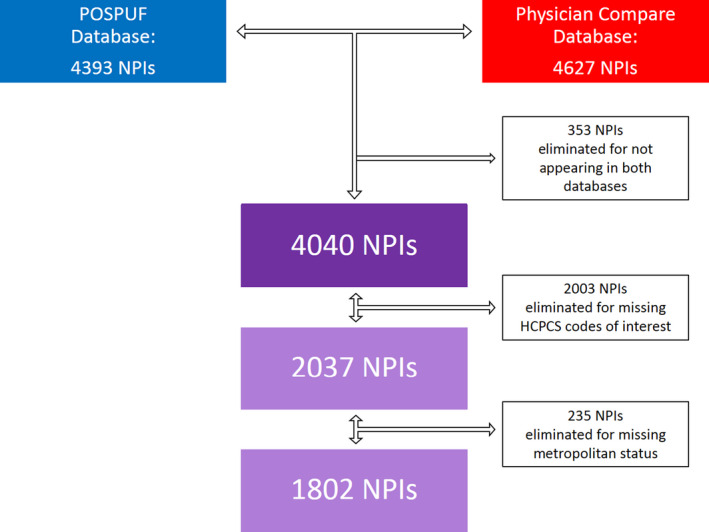
Methods: The Centers for Medicare and Medicaid Services (CMS) Physician and Other Supplier Public Use File was linked to the CMS Physician Compare (PC) database by physician NPI to identify and sum all treatment delivery charges submitted by individual radiation oncologists in the non-facility-based (NFB) setting in 2016. Multivariable logistic regression analysis was carried out to determine provider characteristics (gender, practice rurality, practice region, and years since graduation) that predicted for the delivery of 3D conformal RT (3DCRT), intensity modulated RT (IMRT), stereotactic body RT (SBRT), stereotactic radiosurgery (SRS), low dose rate (LDR) brachytherapy, and high dose rate (HDR) brachytherapy delivery in the Medicare patient population. The overall significance of categorical variables in the multivariable logistic regression model was assessed by the likelihood ratio test (LRT).
Results: In total, 1,802 physicians from the NFB practice setting were analyzed. Male gender predicted for greater LDR brachytherapy delivery (OR 8.19, 95% CI 2.58-26.05, p < 0.001), but not greater delivery of other technologies. Metropolitan practice was the only predictor for greater HDR brachytherapy utilization (OR 12.95, 95% CI 1.81-92.60, p = 0.01). Practice region was predictive of the delivery of 3DCRT, SRS and SBRT (p < 0.01, p < 0.001, and p < 0.001, respectively). With the Northeast as the reference region, 3DCRT was more likely to be delivered by providers in the South (OR 1.33, 95% CI 1.09-1.62, p < 0.01) and the West (OR 1.38, 95% CI 1.11-1.71, p < 0.01). At the same time, SRS use was less likely in the Midwest (OR 0.71, 95% CI 0.55-0.91, p < 0.01), South (OR 0.49, 95% CI 0.40-0.61, p < 0.001), and West (OR 0.43, 95% CI 0.34-0.55, p < 0.001). SBRT, on the other hand, was more commonly utilized in the Midwest (OR 2.63, 95% CI 1.13-6.13, p = 0.03), South (OR 3.44, 95% CI 1.58-7.49, p < 0.01), and West (OR 4.87, 95% CI 2.21-10.72, p < 0.001). HDR brachytherapy use was also more likely in the Midwest (OR 1.97, 95% CI 1.11-3.49, p = 0.02) and West (OR 1.87, 95% CI 1.08-3.24, p = 0.03). While the degree held by the billing physician did not predict for delivery of a given procedure, greater years since graduation was related to decreased likelihood of SBRT use (OR 0.98, 95% CI 0.96-0.99, p < 0.001) and increased likelihood of LDR brachytherapy use (OR 1.02, 95% CI 1.00-1.04, p = 0.02).
Conclusions: Substantial geographic variation in the use of specific RT technologies was identified. The degree to which this variation reflects effective care, preference-sensitive care, or supply-sensitive care warrants further investigation.
Keywords: behavioral science; clinical management; radiation therapy; radiotherapy; registries.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
Similar articles
-
Provider-Level Variation in Treatment Planning of Radiation Oncology Procedures in the United States.JCO Oncol Pract. 2021 Dec;17(12):e1905-e1912. doi: 10.1200/OP.20.00441. Epub 2021 Jan 8. JCO Oncol Pract. 2021. PMID: 33417480
-
Provider variability in intensity modulated radiation therapy utilization among Medicare beneficiaries in the United States.Pract Radiat Oncol. 2018 Sep-Oct;8(5):e329-e336. doi: 10.1016/j.prro.2018.02.004. Epub 2018 Feb 16. Pract Radiat Oncol. 2018. PMID: 29861349
-
Assessment of Differences in Clinical Activity and Medicare Payments Among Female and Male Radiation Oncologists.JAMA Netw Open. 2019 Mar 1;2(3):e190932. doi: 10.1001/jamanetworkopen.2019.0932. JAMA Netw Open. 2019. PMID: 30901047 Free PMC article.
-
Advances in Radiation Oncology for the Treatment of Cervical Cancer.Curr Oncol. 2022 Feb 9;29(2):928-944. doi: 10.3390/curroncol29020079. Curr Oncol. 2022. PMID: 35200578 Free PMC article. Review.
-
[Recent developments in radiation oncology-integrating radiation physics and molecular radiobiology advances into clinical radiotherapy practice and beyond].Ai Zheng. 2008 Aug;27(8):885-93. Ai Zheng. 2008. PMID: 18710628 Review. Chinese.
Cited by
-
Radiation Oncology Virtual Education Rotation (ROVER) 2.0 for Residents: Implementation and Outcomes.J Cancer Educ. 2023 Jun;38(3):977-984. doi: 10.1007/s13187-022-02216-1. Epub 2022 Sep 9. J Cancer Educ. 2023. PMID: 36083458 Free PMC article.
References
-
- Wennberg JE. Forty years of unwarranted variation–and still counting. Health Policy Amst Neth. 2014;114(1):1‐2. - PubMed
-
- Curfman G, Shachar C, Navathe A. Beyond the Dartmouth Atlas ‐ regional variation in private health care spending. Healthc Amst Neth. 2016;4(3):132‐134. - PubMed
-
- Hyams E, Goodney P, Dzebisashvili N, Goodman D, Bronner K . Variation in the Care of Surgical Conditions: Prostate Cancer [Internet]. The Dartmouth Institute of Health Policy & Clinical Practice; 2014. Dec [cited 2019 Aug 23] p. 50. Available from: http://archive.dartmouthatlas.org/downloads/reports/Prostate_cancer_repo... - PubMed
-
- Delaney G, Jacob S, Featherstone C, Barton M. The role of radiotherapy in cancer treatment: estimating optimal utilization from a review of evidence‐based clinical guidelines. Cancer. 2005;104(6):1129‐1137. - PubMed
-
- Proposed Radiation Oncology (RO) Model | CMS [Internet]. [cited 2020 Jan 11]. Available from: https://www.cms.gov/newsroom/fact‐sheets/proposed‐radiation‐oncology‐ro‐...
