

Rotational Thromboelastometry Findings Are Associated with Symptomatic Venous Thromboembolic Complications after Hip Fracture Surgery
- PMID: 34076610
- PMCID: PMC8509944
- DOI: 10.1097/CORR.0000000000001832
Rotational Thromboelastometry Findings Are Associated with Symptomatic Venous Thromboembolic Complications after Hip Fracture Surgery
Abstract
Background: Venous thromboembolism is a common complication after hip fractures. However, there are no reliable laboratory assays to identify patients at risk for venous thromboembolic (VTE) events after major orthopaedic surgery.
Question/purposes: (1) Are rotational thromboelastometry (ROTEM) findings associated with the presence or development of symptomatic VTE after hip fracture surgery? (2) Were any other patient factors associated with the presence or development of symptomatic VTE after hip fracture surgery? (3) Which ROTEM parameters were the most accurate in terms of detecting the association of hypercoagulability with symptomatic VTE?
Methods: This retrospective study was conducted over a 13-month period. In all, 354 patients with femoral neck and peritrochanteric fractures who underwent hip hemiarthoplasty or cephallomedullary nailing were assessed for eligibility. Of those, 99% (349 of 354) were considered eligible for the study, 1% (3 of 354) of patients were excluded due to coagulation disorders, and another 1% (2 of 354) were excluded because they died before the postoperative ROTEM analysis. An additional 4% (13 of 354) of patients were lost before the minimum study follow-up of 3 months, leaving 95% (336 of 354) for analysis. A ROTEM analysis was performed in all patients at the time of their hospital admission, within hours of the injury, and on the second postoperative day. The patients were monitored for the development of symptoms indicative of VTE, and the gold standard tests for diagnosing VTE, such as CT pulmonary angiography or vascular ultrasound, were selectively performed only in symptomatic patients and not routinely in all patients. Therefore, this study evaluates the association of ROTEM with only clinically evident VTE events and not with all VTE events. ROTEM results did not affect the clinical surveillance of the study group and the decision for further work up. To determine whether ROTEM findings were associated with the presence or development of symptomatic VTE, ROTEM parameters were compared between patients with and without symptomatic VTE. To establish whether any other patient factors were associated with the presence or development of symptomatic VTE after hip fracture surgery, clinical parameters and conventional laboratory values were also compared between patients with and without symptomatic VTE. Finally, to determine which ROTEM parameters were the most accurate in terms of detecting the association of hypercoagulability with symptomatic VTE, the area under the curve (AUC) for certain cut off values of ROTEM parameters was calculated.
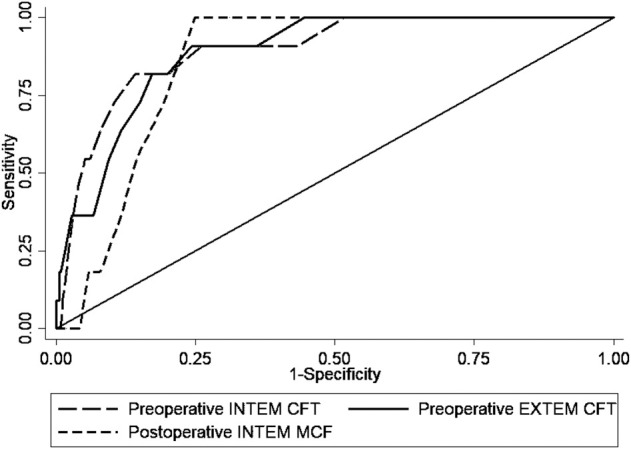
Results: We found several abnormal ROTEM values to be associated with the presence or development of symptomatic VTE. The preoperative maximum clot firmness was higher in patients with clinically evident VTE than in patients without these complications (median [interquartile range] 70 mm [68 to 71] versus 65 mm [61 to 68]; p < 0.001). The preoperative clot formation time was lower in patients with clinically evident VTE than those without clinically evident VTE (median 61 seconds [58 to 65] versus 70 seconds [67 to 74]; p < 0.001), and also the postoperative clot formation time was lower in patients with clinically evident VTE than those without these complications (median 52 seconds [49 to 59] versus 62 seconds [57 to 68]; p < 0.001). Increased BMI was also associated with clinically evident VTE (odds ratio 1.26 [95% confidence interval 1.07 to 1.53]; p < 0.001). We found no differences between patients with and without clinically evident VTE in terms of age, sex, smoking status, comorbidities, and preoperative use of anticoagulants. Lastly, preoperative clot formation time demonstrated the best performance for detecting the association of hypercoagulability with symptomatic VTE (AUC 0.89 [95% CI 0.81 to 0.97]), with 81% (95% CI 48% to 97%) sensitivity and 86% (95% CI 81% to 89%) specificity for clot formation time ≤ 65 seconds.
Conclusion: ROTEM's performance in this preliminary study was promising in terms of its association with symptomatic VTE. This study extended our earlier work by demonstrating that ROTEM has a high accuracy in detecting the level of hypercoagulability that is associated with symptomatic VTE. However, until its performance is validated in a study that applies a diagnostic gold standard (such as venography, duplex/Doppler, or chest CT) in all patients having ROTEM to confirm its performance, ROTEM should not be used as a regular part of clinical practice.
Level of evidence: Level IV, diagnostic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that neither he nor she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: Rotational Thromboelastometry Findings Are Associated with Symptomatic Venous Thromboembolic Complications after Hip Fracture Surgery.Clin Orthop Relat Res. 2021 Nov 1;479(11):2468-2470. doi: 10.1097/CORR.0000000000001961. Clin Orthop Relat Res. 2021. PMID: 34448732 Free PMC article. No abstract available.
Similar articles
-
What Proportion of Patients With Musculoskeletal Tumors Demonstrate Thromboelastographic Markers of Hypercoagulability? A Pilot Study.Clin Orthop Relat Res. 2023 Mar 1;481(3):553-561. doi: 10.1097/CORR.0000000000002314. Epub 2022 Jul 12. Clin Orthop Relat Res. 2023. PMID: 35901446 Free PMC article.
-
Rotational thromboelastometry predicts thromboembolic complications after major non-cardiac surgery.Crit Care. 2014 Oct 8;18(5):549. doi: 10.1186/s13054-014-0549-2. Crit Care. 2014. PMID: 25292221 Free PMC article.
-
Fibrinolysis shutdown and elevated D-dimer levels have high prognostic capacity for postoperative thromboembolic complications in patients with bone tumors.J Thromb Thrombolysis. 2023 Apr;55(3):536-544. doi: 10.1007/s11239-023-02787-w. Epub 2023 Feb 26. J Thromb Thrombolysis. 2023. PMID: 36843157
-
Ability of Thromboelastography to Detect Hypercoagulability: A Systematic Review and Meta-Analysis.J Orthop Trauma. 2020 Jun;34(6):278-286. doi: 10.1097/BOT.0000000000001714. J Orthop Trauma. 2020. PMID: 31815829
-
Rivaroxaban versus aspirin in prevention of venous thromboembolism following total joint arthroplasty or hip fracture surgery: a meta-analysis.J Orthop Surg Res. 2021 Feb 13;16(1):135. doi: 10.1186/s13018-021-02274-z. J Orthop Surg Res. 2021. PMID: 33581718 Free PMC article. Review.
Cited by
-
Patients with infective endocarditis undergoing cardiac surgery have distinct ROTEM profiles and more bleeding complications compared to patients without infective endocarditis.PLoS One. 2023 Apr 13;18(4):e0284329. doi: 10.1371/journal.pone.0284329. eCollection 2023. PLoS One. 2023. PMID: 37053130 Free PMC article.
-
Enhanced diagnostic capabilities of thromboelastography coupled with standard coagulation indices for predicting perioperative thrombosis in older individuals with hip fractures : TEG coupled with standard coagulation indices for predicting thrombosis in hip fractures.J Orthop Surg Res. 2024 Dec 24;19(1):870. doi: 10.1186/s13018-024-05386-4. J Orthop Surg Res. 2024. PMID: 39719587 Free PMC article.
-
The Acute and Chronic Effects of Resistance and Aerobic Exercise in Hemostatic Balance: A Brief Review.Sports (Basel). 2023 Mar 27;11(4):74. doi: 10.3390/sports11040074. Sports (Basel). 2023. PMID: 37104148 Free PMC article. Review.
-
Impaired fibrinolysis and increased clot strength are potential risk factors for thrombosis in lymphoma.Blood Adv. 2023 Nov 28;7(22):7056-7066. doi: 10.1182/bloodadvances.2023011379. Blood Adv. 2023. PMID: 37756519 Free PMC article.
-
Red Cell Distribution Width-to-High-Density Lipoprotein Cholesterol Ratio (RHR): A Promising Novel Predictor for Preoperative Deep Vein Thrombosis in Geriatric Patients with Hip Fracture.Clin Interv Aging. 2022 Sep 1;17:1319-1329. doi: 10.2147/CIA.S375762. eCollection 2022. Clin Interv Aging. 2022. PMID: 36072306 Free PMC article.
References
-
- Anderson FA, Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation . 2003;107:I9-I16. - PubMed
-
- Berquist D, Efsing HO, Hallbook T, Hedlund T. Thromboembolism after elective and post-traumatic hip surgery—a controlled prophylactic trial with dextran 70 and low-dose heparin. Acta Chir Scand . 1979;145:213-218. - PubMed
-
- Brown W, Lunati M, Maceroli M, et al. Ability of thromboelastography to detect hypercoagulability: a systematic review and meta-analysis. J Orthop Trauma . 2020;34:278-286. - PubMed
-
- Connelly C, Van P, Hart K, et al. Thrombelastography-based dosing of enoxaparin for thromboprophylaxis in trauma and surgical patients. JAMA Surg. 2016;151:e162069. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
