

Association of Opioid Agonist Treatment With All-Cause Mortality and Specific Causes of Death Among People With Opioid Dependence: A Systematic Review and Meta-analysis
- PMID: 34076676
- PMCID: PMC8173472
- DOI: 10.1001/jamapsychiatry.2021.0976
Association of Opioid Agonist Treatment With All-Cause Mortality and Specific Causes of Death Among People With Opioid Dependence: A Systematic Review and Meta-analysis
Erratum in
-
Error in Abstract.JAMA Psychiatry. 2021 Sep 1;78(9):1044. doi: 10.1001/jamapsychiatry.2021.1754. JAMA Psychiatry. 2021. PMID: 34190969 Free PMC article. No abstract available.
-
Error in Abstract.JAMA Psychiatry. 2022 May 1;79(5):516. doi: 10.1001/jamapsychiatry.2022.0357. JAMA Psychiatry. 2022. PMID: 35293962 Free PMC article. No abstract available.
-
Errors in Results and Tables.JAMA Psychiatry. 2023 Sep 1;80(9):972. doi: 10.1001/jamapsychiatry.2023.2537. JAMA Psychiatry. 2023. PMID: 37466992 Free PMC article. No abstract available.
Abstract
Importance: Mortality among people with opioid dependence is higher than that of the general population. Opioid agonist treatment (OAT) is an effective treatment for opioid dependence; however, there has not yet been a systematic review on the relationship between OAT and specific causes of mortality.
Objective: To estimate the association of time receiving OAT with mortality.
Data sources: The Embase, MEDLINE, and PsycINFO databases were searched through February 18, 2020, including clinical trial registries and previous Cochrane reviews.
Study selection: All observational studies that collected data on all-cause or cause-specific mortality among people with opioid dependence while receiving and not receiving OAT were included. Randomized clinical trials (RCTs) were also included.
Data extraction and synthesis: This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. Data on study, participant, and treatment characteristics were extracted; person-years, all-cause mortality, and cause-specific mortality were calculated. Crude mortality rates and rate ratios (RRs) were pooled using random-effects meta-analyses.
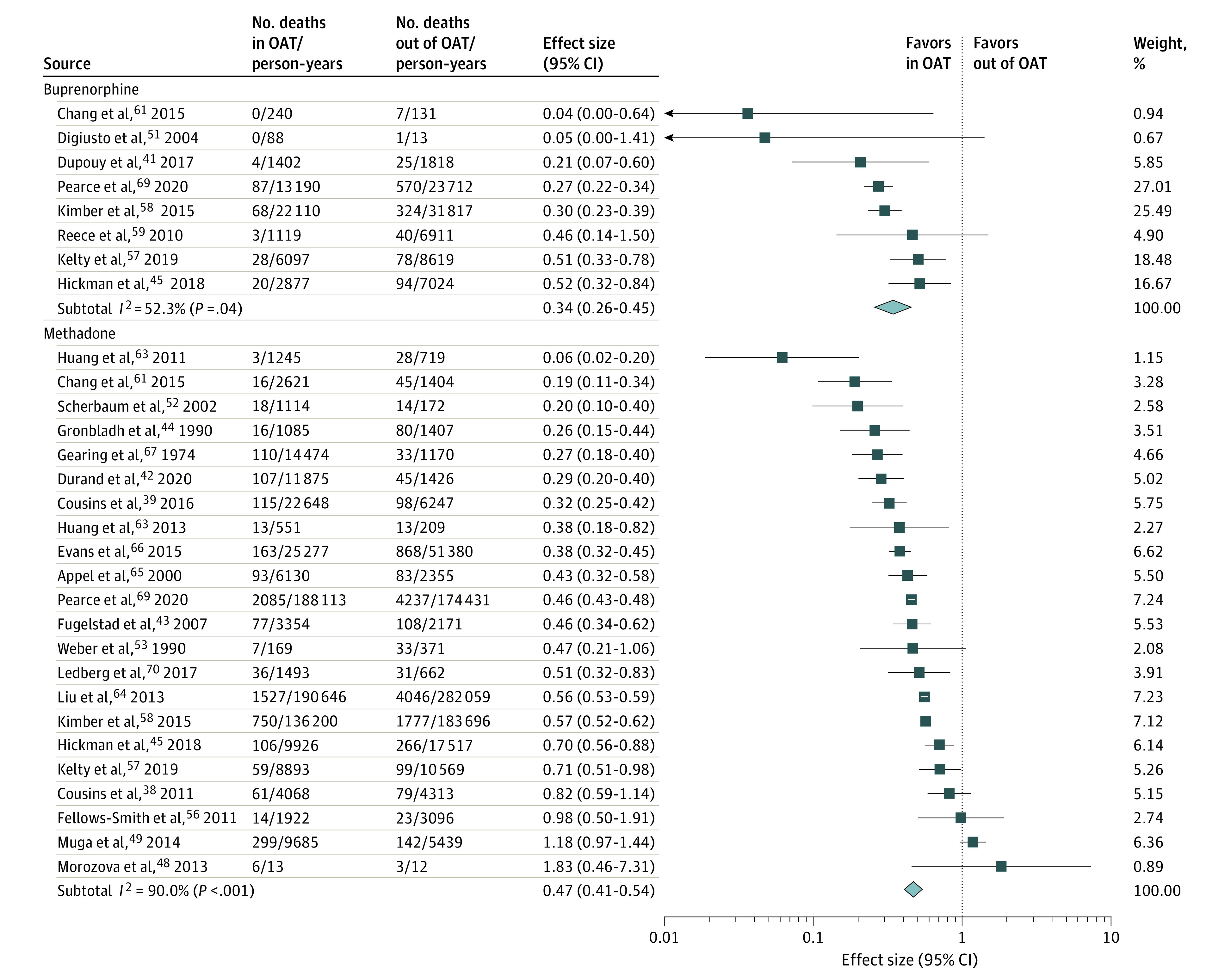
Main outcomes and measures: Overall all-cause and cause-specific mortality both by setting and by participant characteristics. Methadone and buprenorphine OAT were evaluated specifically.
Results: Fifteen RCTs including 3852 participants and 36 primary cohort studies including 749 634 participants were analyzed. Among the cohort studies, the rate of all-cause mortality during OAT was more than half of the rate seen during time out of OAT (RR, 0.47; 95% CI, 0.42-0.53). This association was consistent regardless of patient sex, age, geographic location, HIV status, and hepatitis C virus status and whether drugs were taken through injection. Associations were not different for methadone (RR, 0.47; 95% CI, 0.41-0.54) vs buprenorphine (RR, 0.34; 95% CI, 0.26-0.45). There was lower risk of suicide (RR, 0.48; 95% CI, 0.37-0.61), cancer (RR, 0.72; 95% CI, 0.52-0.98), drug-related (RR, 0.41; 95% CI, 0.33-0.52), alcohol-related (RR, 0.59; 95% CI, 0.49-0.72), and cardiovascular-related (RR, 0.69; 95% CI, 0.60-0.79) mortality during OAT. In the first 4 weeks of methadone treatment, rates of all-cause mortality and drug-related poisoning were almost double the rates during the remainder of OAT (RR, 2.01; 95% CI, 1.55-5.09) but not for buprenorphine (RR, 0.58; 95% CI, 0.18-1.85). All-cause mortality was 6 times higher in the 4 weeks after OAT cessation (RR, 6.01; 95% CI, 4.32-8.36), remaining double the rate for the remainder of time not receiving OAT (RR, 1.81; 95% CI, 1.50-2.18). Opioid agonist treatment was associated with a lower risk of mortality during incarceration (RR, 0.06; 95% CI, 0.01-0.46) and after release from incarceration (RR, 0.09; 95% CI, 0.02-0.56).
Conclusions and relevance: This systematic review and meta-analysis found that OAT was associated with lower rates of mortality. However, access to OAT remains limited, and coverage of OAT remains low. Work to improve access globally may have important population-level benefits.
Conflict of interest statement
Figures
Comment in
-
Errors in Data Reported in Meta-Analysis on Opioid Agonist Treatment and Mortality.JAMA Psychiatry. 2023 Sep 1;80(9):971-972. doi: 10.1001/jamapsychiatry.2023.2342. JAMA Psychiatry. 2023. PMID: 37466957 No abstract available.
