

An enhanced therapeutic effect of repetitive transcranial magnetic stimulation combined with antibody treatment in a primate model of spinal cord injury
- PMID: 34077429
- PMCID: PMC8172028
- DOI: 10.1371/journal.pone.0252023
An enhanced therapeutic effect of repetitive transcranial magnetic stimulation combined with antibody treatment in a primate model of spinal cord injury
Abstract
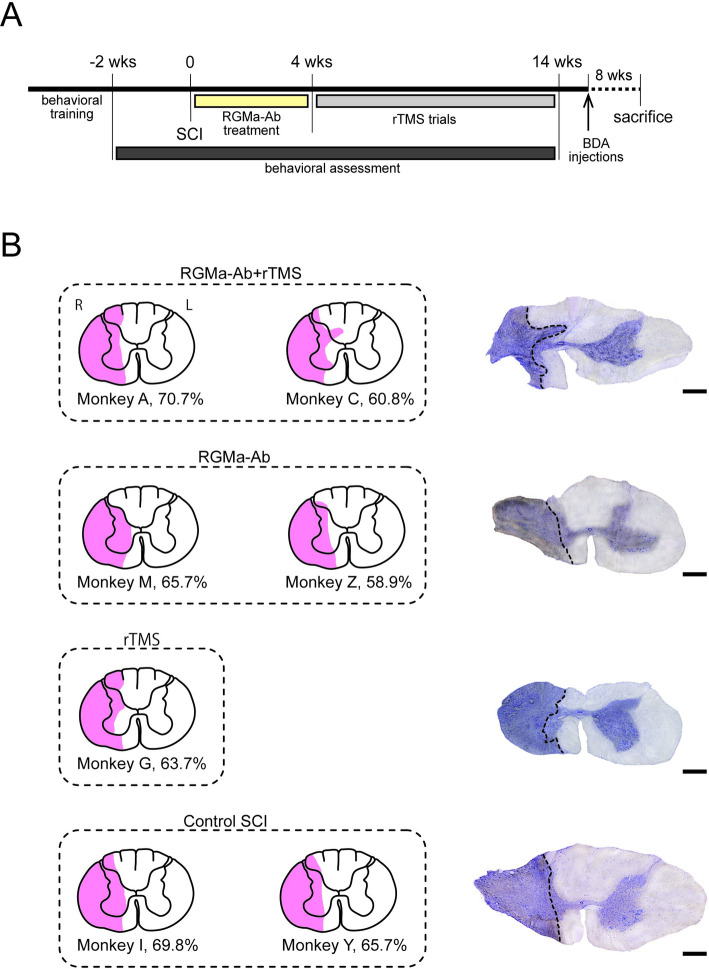
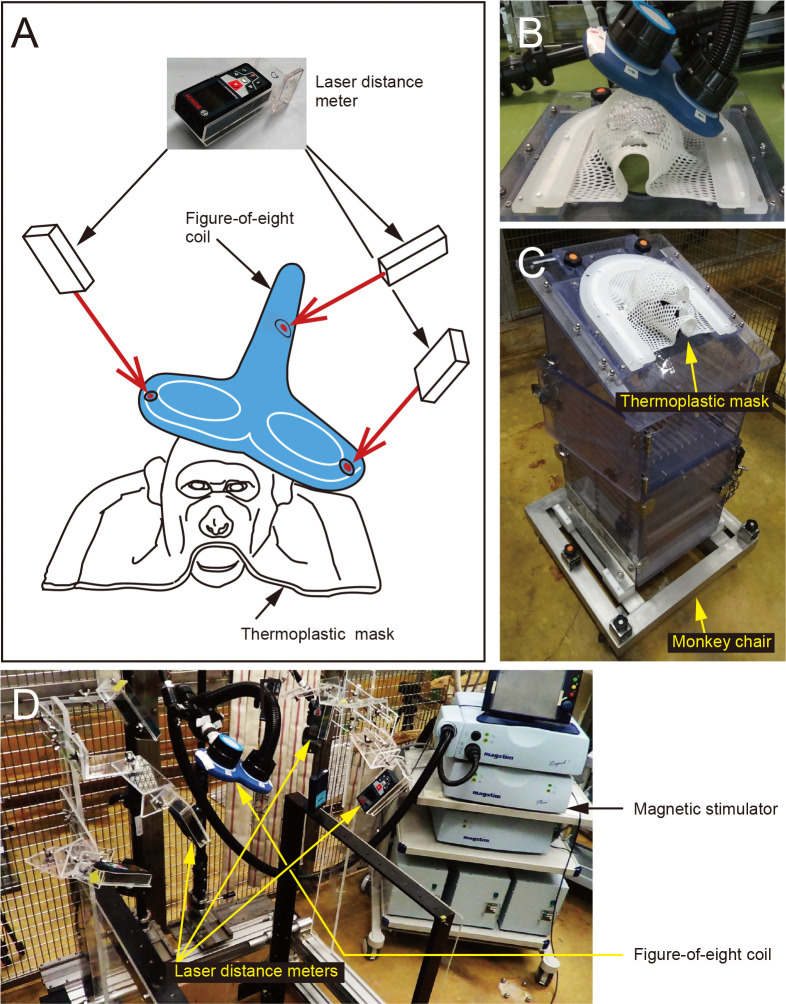
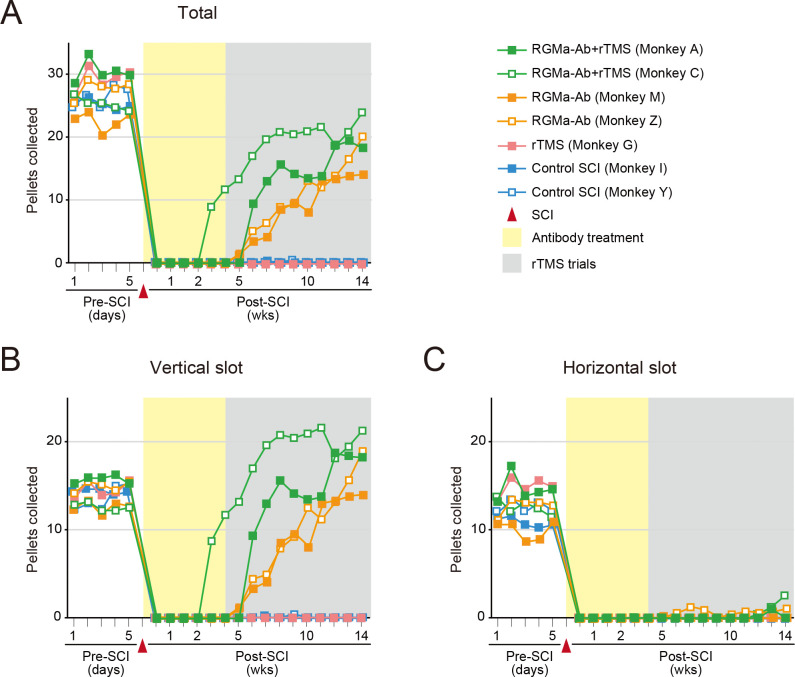
Repetitive transcranial magnetic stimulation (rTMS) targeting the primary motor cortex (MI) is expected to provide a therapeutic impact on spinal cord injury (SCI). On the other hand, treatment with antibody against repulsive guidance molecule-a (RGMa) has been shown to ameliorate motor deficits after SCI in rodents and primates. Facilitating activity of the corticospinal tract (CST) by rTMS following rewiring of CST fibers by anti-RGMa antibody treatment may exert an enhanced effect on motor recovery in a primate model of SCI. To address this issue, we examined whether such a combined therapeutic strategy could contribute to accelerating functional restoration from SCI. In our SCI model, unilateral lesions were made between the C6 and the C7 level. Two macaque monkeys were used for each of the combined therapy and antibody treatment alone, while one monkey was for rTMS alone. The antibody treatment was continuously carried out for four weeks immediately after SCI, and rTMS trials applying a thermoplastic mask and a laser distance meter lasted ten weeks. Behavioral assessment was performed over 14 weeks after SCI to investigate the extent to which motor functions were restored with the antibody treatment and/or rTMS. While rTMS without the preceding antibody treatment produced no discernible sign for functional recovery, a combination of the antibody and rTMS exhibited a greater effect, especially at an early stage of rTMS trials, on restoration of dexterous hand movements. The present results indicate that rTMS combined with anti-RGMa antibody treatment may exert a synergistic effect on motor recovery from SCI.
Conflict of interest statement
The authors have read the journal’s policy and have the following competing interests: Mitsubishi Tanabe Pharma Corporation provided financial support for the study in the form of funding for the expendables and a stipend awarded to HY and MT, as well as material support in the form of the anti-RGMa antibody used in the study. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no other patents, products in development or marketed products associated with this research to declare.
Figures
Similar articles
-
Anti-repulsive guidance molecule-a antibody treatment and repetitive transcranial magnetic stimulation have synergistic effects on motor recovery after spinal cord injury.Neurosci Lett. 2019 Sep 14;709:134329. doi: 10.1016/j.neulet.2019.134329. Epub 2019 Jun 11. Neurosci Lett. 2019. PMID: 31200090
-
Elezanumab, a human anti-RGMa monoclonal antibody, promotes neuroprotection, neuroplasticity, and neurorecovery following a thoracic hemicompression spinal cord injury in non-human primates.Neurobiol Dis. 2021 Jul;155:105385. doi: 10.1016/j.nbd.2021.105385. Epub 2021 May 12. Neurobiol Dis. 2021. PMID: 33991647
-
Treatment With the Neutralizing Antibody Against Repulsive Guidance Molecule-a Promotes Recovery From Impaired Manual Dexterity in a Primate Model of Spinal Cord Injury.Cereb Cortex. 2019 Feb 1;29(2):561-572. doi: 10.1093/cercor/bhx338. Cereb Cortex. 2019. PMID: 29315368
-
Effects of repetitive transcranial magnetic stimulation on recovery of function after spinal cord injury.Arch Phys Med Rehabil. 2015 Apr;96(4 Suppl):S145-55. doi: 10.1016/j.apmr.2014.07.418. Epub 2014 Aug 29. Arch Phys Med Rehabil. 2015. PMID: 25175159 Free PMC article. Review.
-
Repetitive Transcranial Magnetic Stimulation for the Treatment of Spinal Cord Injury: Current Status and Perspective.Int J Mol Sci. 2025 Jan 19;26(2):825. doi: 10.3390/ijms26020825. Int J Mol Sci. 2025. PMID: 39859537 Free PMC article. Review.
Cited by
-
Combinatorial therapies for spinal cord injury repair.Neural Regen Res. 2025 May 1;20(5):1293-1308. doi: 10.4103/NRR.NRR-D-24-00061. Epub 2024 Jun 3. Neural Regen Res. 2025. PMID: 38845223 Free PMC article.
-
Research progress on the application of transcranial magnetic stimulation in spinal cord injury rehabilitation: a narrative review.Front Neurol. 2023 Jul 18;14:1219590. doi: 10.3389/fneur.2023.1219590. eCollection 2023. Front Neurol. 2023. PMID: 37533475 Free PMC article. Review.
-
Exosomes derived from CD271+CD56+ bone marrow mesenchymal stem cell subpopoulation identified by single-cell RNA sequencing promote axon regeneration after spinal cord injury.Theranostics. 2024 Jan 1;14(2):510-527. doi: 10.7150/thno.89008. eCollection 2024. Theranostics. 2024. PMID: 38169566 Free PMC article.
-
circ_014260/miR-384/THBS1 aggravates spinal cord injury in rats by promoting neuronal apoptosis and endoplasmic reticulum stress.Am J Transl Res. 2022 Jan 15;14(1):518-533. eCollection 2022. Am J Transl Res. 2022. PMID: 35173872 Free PMC article.
-
Repulsive Guidance Molecule-A as a Therapeutic Target Across Neurological Disorders: An Update.Int J Mol Sci. 2025 Mar 30;26(7):3221. doi: 10.3390/ijms26073221. Int J Mol Sci. 2025. PMID: 40244061 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
