

COVID-19: Seroprevalence and Vaccine Responses in UK Dental Care Professionals
- PMID: 34077690
- PMCID: PMC8461044
- DOI: 10.1177/00220345211020270
COVID-19: Seroprevalence and Vaccine Responses in UK Dental Care Professionals
Abstract
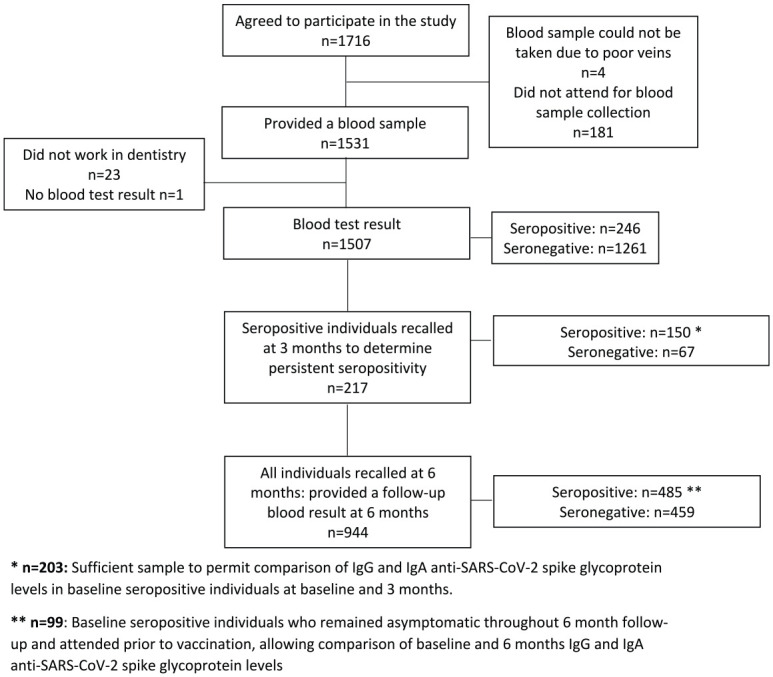
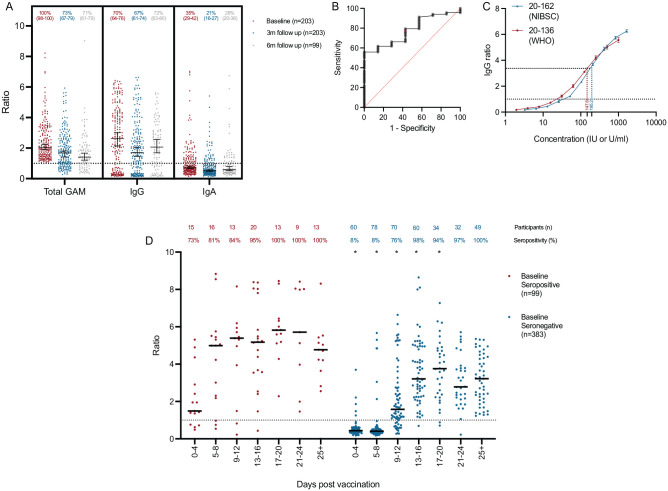
Dental care professionals (DCPs) are thought to be at enhanced risk of occupational exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). However, robust data to support this from large-scale seroepidemiological studies are lacking. We report a longitudinal seroprevalence analysis of antibodies to SARS-CoV-2 spike glycoprotein, with baseline sampling prior to large-scale practice reopening in July 2020 and follow-up postimplementation of new public health guidance on infection prevention control (IPC) and enhanced personal protective equipment (PPE). In total, 1,507 West Midlands DCPs were recruited into this study in June 2020. Baseline seroprevalence was determined using a combined IgGAM enzyme-linked immunosorbent assay and the cohort followed longitudinally for 6 mo until January/February 2021 through the second wave of the coronavirus disease 2019 pandemic in the United Kingdom and vaccination commencement. Baseline seroprevalence was 16.3%, compared to estimates in the regional population of 6% to 7%. Seropositivity was retained in over 70% of participants at 3- and 6-mo follow-up and conferred a 75% reduced risk of infection. Nonwhite ethnicity and living in areas of greater deprivation were associated with increased baseline seroprevalence. During follow-up, no polymerase chain reaction-proven infections occurred in individuals with a baseline anti-SARS-CoV-2 IgG level greater than 147.6 IU/ml with respect to the World Health Organization international standard 20-136. After vaccination, antibody responses were more rapid and of higher magnitude in those individuals who were seropositive at baseline. Natural infection with SARS-CoV-2 prior to enhanced PPE was significantly higher in DCPs than the regional population. Natural infection leads to a serological response that remains detectable in over 70% of individuals 6 mo after initial sampling and 9 mo from the peak of the first wave of the pandemic. This response is associated with protection from future infection. Even if serological responses wane, a single dose of the Pfizer-BioNTech 162b vaccine is associated with an antibody response indicative of immunological memory.
Keywords: SARS-CoV-2; antibodies; dentistry; occupational exposure; seroepidemiological studies; vaccination.
Conflict of interest statement
Figures
Comment in
-
Seroprevalence and vaccine responses.Br Dent J. 2021 Jun;230(12):822. doi: 10.1038/s41415-021-3177-7. Br Dent J. 2021. PMID: 34172867 Free PMC article. No abstract available.
References
-
- Allison JR, Currie CC, Edwards DC, Bowes C, Coulter J, Pickering K, Kozhevnikova E, Durham J, Nile CJ, Jakubovics N, et al.. 2021. Evaluating aerosol and splatter following dental procedures: addressing new challenges for oral health care and rehabilitation. J Oral Rehabil. 48(1):61–72. - PMC - PubMed
-
- Cook AM, Faustini SE, Williams LJ, Cunningham AF, Drayson MT, Shields AM, Kay D, Taylor L, Plant T, Huissoon A, et al.. 2021. Validation of a combined ELISA to detect IgG, IgA and IgM antibody responses to SARS-CoV-2 in mild or moderate non-hospitalised patients. J Immunol Methods. 494:113046. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
