

Therapeutic implications of improved molecular diagnostics for rare CNS embryonal tumor entities: results of an international, retrospective study
- PMID: 34077956
- PMCID: PMC8408859
- DOI: 10.1093/neuonc/noab136
Therapeutic implications of improved molecular diagnostics for rare CNS embryonal tumor entities: results of an international, retrospective study
Abstract
Background: Only few data are available on treatment-associated behavior of distinct rare CNS embryonal tumor entities previously treated as "CNS-primitive neuroectodermal tumors" (CNS-PNET). Respective data on specific entities, including CNS neuroblastoma, FOXR2 activated (CNS NB-FOXR2), and embryonal tumors with multilayered rosettes (ETMR) are needed for development of differentiated treatment strategies.
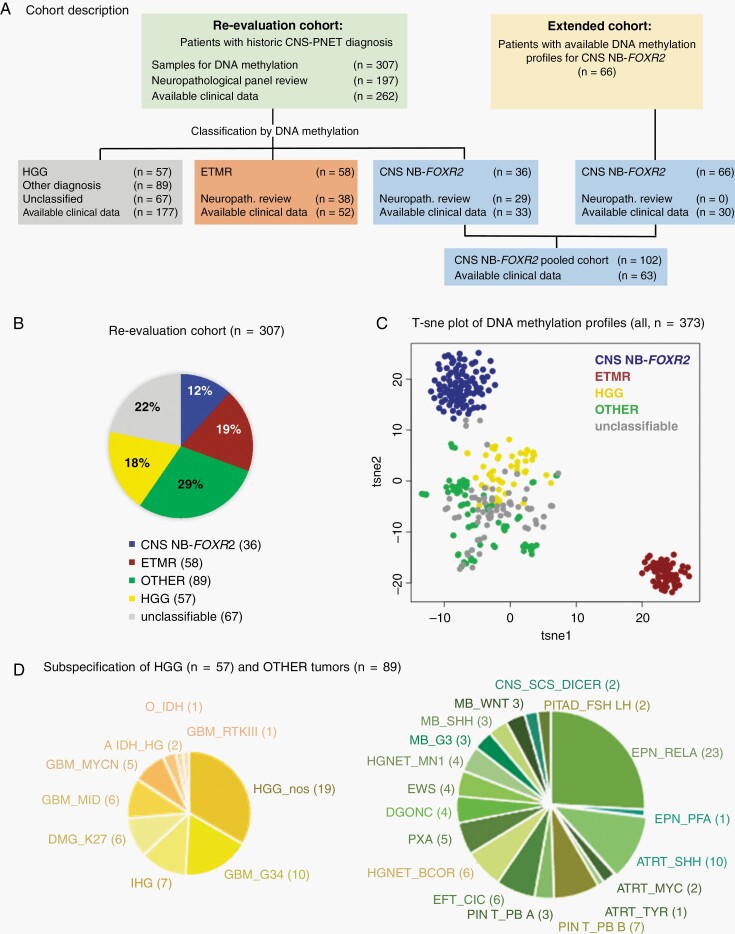
Methods: Within this retrospective, international study, tumor samples of clinically well-annotated patients with the original diagnosis of CNS-PNET were analyzed using DNA methylation arrays (n = 307). Additional cases (n = 66) with DNA methylation pattern of CNS NB-FOXR2 were included irrespective of initial histological diagnosis. Pooled clinical data (n = 292) were descriptively analyzed.
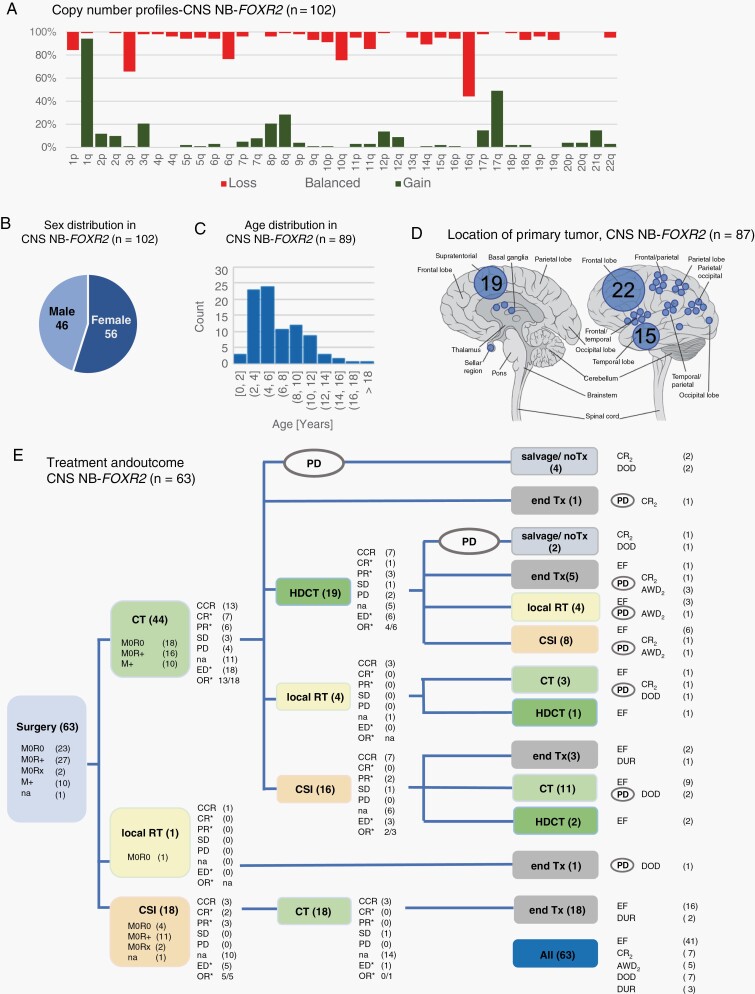
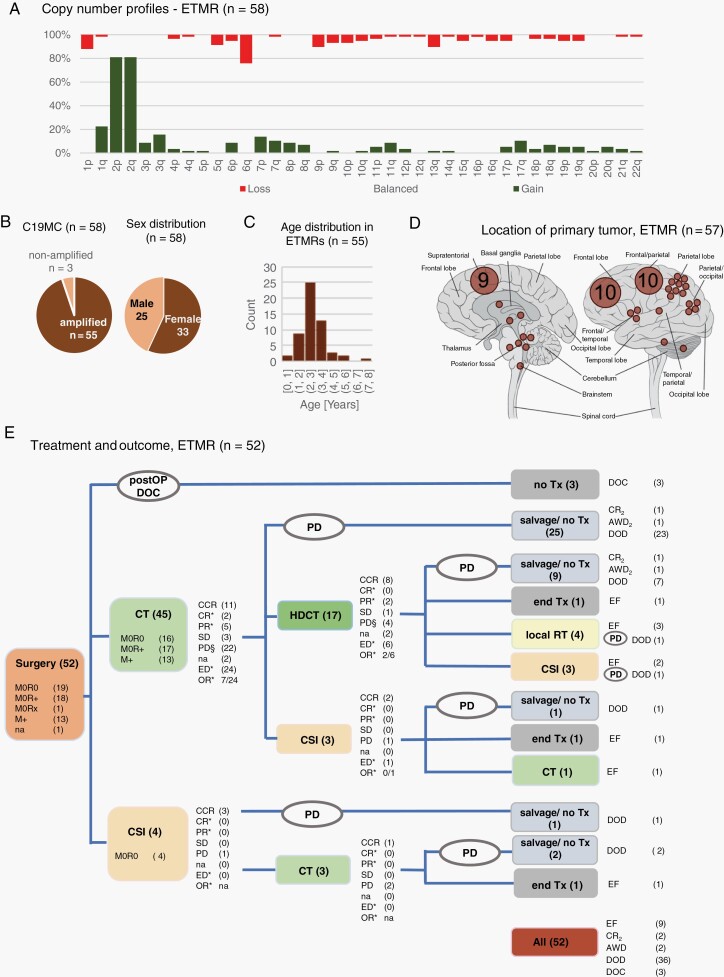
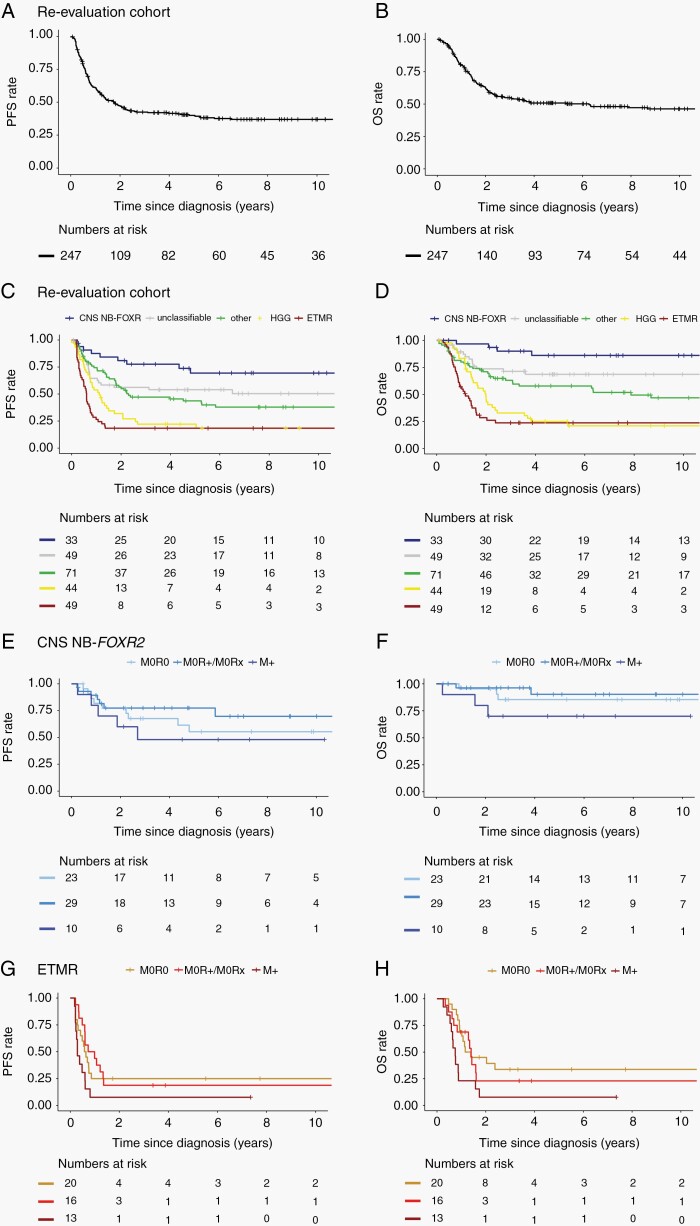
Results: DNA methylation profiling of "CNS-PNET" classified 58 (19%) cases as ETMR, 57 (19%) as high-grade glioma (HGG), 36 (12%) as CNS NB-FOXR2, and 89(29%) cases were classified into 18 other entities. Sixty-seven (22%) cases did not show DNA methylation patterns similar to established CNS tumor reference classes. Best treatment results were achieved for CNS NB-FOXR2 patients (5-year PFS: 63% ± 7%, OS: 85% ± 5%, n = 63), with 35/42 progression-free survivors after upfront craniospinal irradiation (CSI) and chemotherapy. The worst outcome was seen for ETMR and HGG patients with 5-year PFS of 18% ± 6% and 22% ± 7%, and 5-year OS of 24% ± 6% and 25% ± 7%, respectively.
Conclusion: The historically reported poor outcome of CNS-PNET patients becomes highly variable when tumors are molecularly classified based on DNA methylation profiling. Patients with CNS NB-FOXR2 responded well to current treatments and a standard-risk CSI-based regimen may be prospectively evaluated. The poor outcome of ETMR across applied treatment strategies substantiates the necessity for evaluation of novel treatments.
Keywords: CNS NB-FOXR2; CNS embryonal tumor; CNS-PNET; DNA methylation profiling; ETMR.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler O, et al. . WHO Classification of Tumours of the Central Nervous System. Revised 4th ed. Lyon: International Agency for Research on Cancer; 2016.
-
- Schwalbe EC, Hayden JT, Rogers HA, et al. . Histologically defined central nervous system primitive neuro-ectodermal tumours (CNS-PNETs) display heterogeneous DNA methylation profiles and show relationships to other paediatric brain tumour types. Acta Neuropathol. 2013;126(6):943–946. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
