

Public health utility of cause of death data: applying empirical algorithms to improve data quality
- PMID: 34078366
- PMCID: PMC8170729
- DOI: 10.1186/s12911-021-01501-1
Public health utility of cause of death data: applying empirical algorithms to improve data quality
Abstract
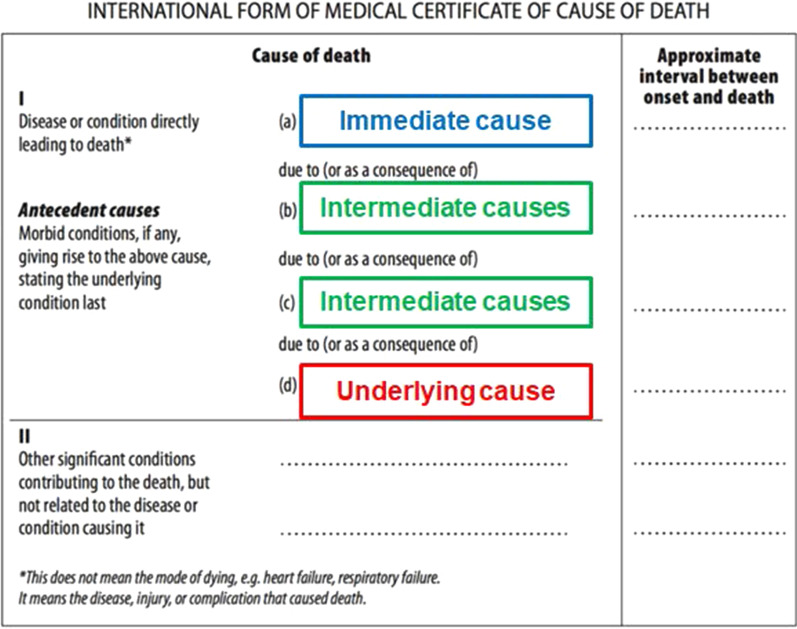
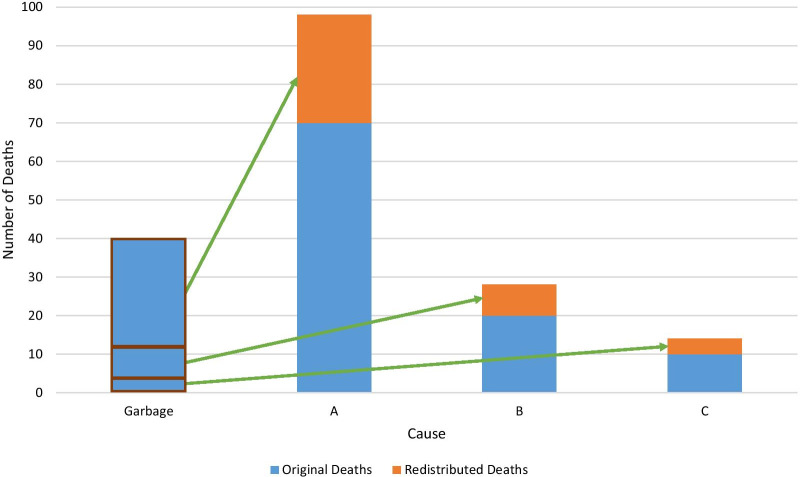
Background: Accurate, comprehensive, cause-specific mortality estimates are crucial for informing public health decision making worldwide. Incorrectly or vaguely assigned deaths, defined as garbage-coded deaths, mask the true cause distribution. The Global Burden of Disease (GBD) study has developed methods to create comparable, timely, cause-specific mortality estimates; an impactful data processing method is the reallocation of garbage-coded deaths to a plausible underlying cause of death. We identify the pattern of garbage-coded deaths in the world and present the methods used to determine their redistribution to generate more plausible cause of death assignments.
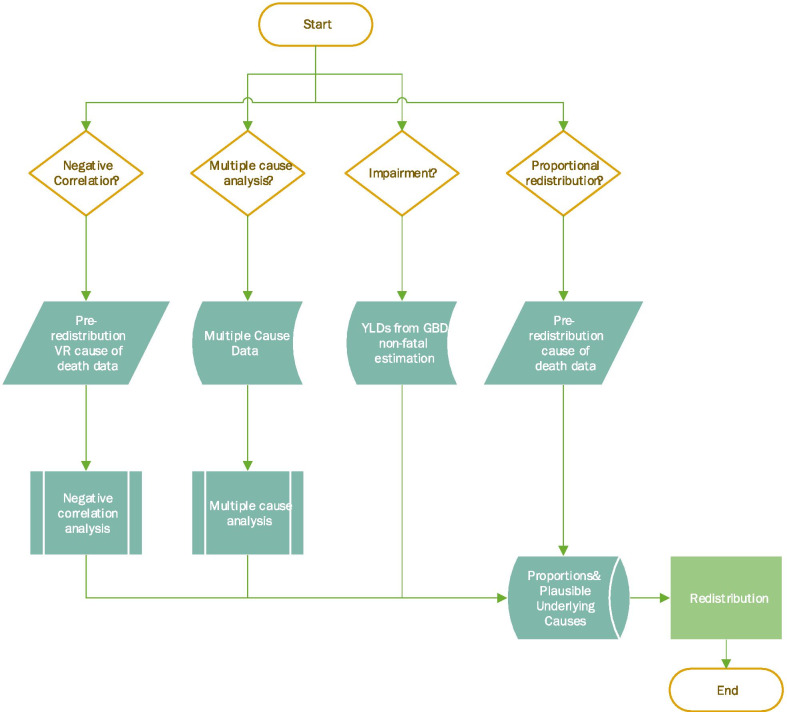
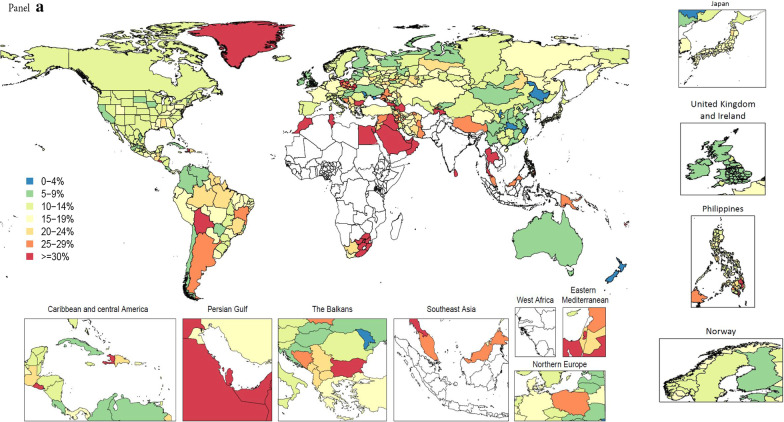
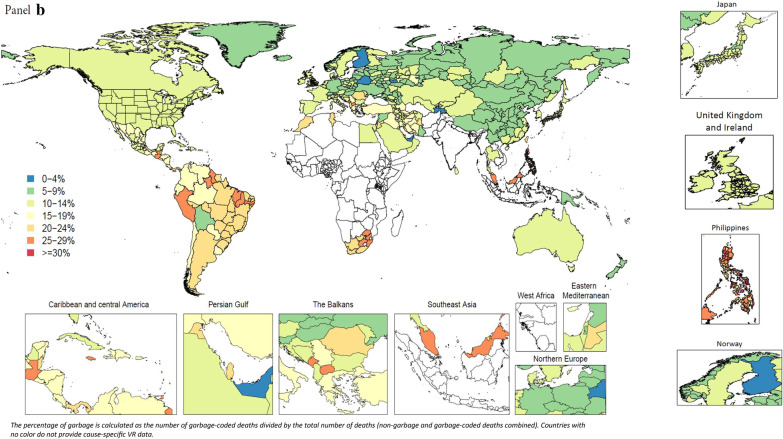
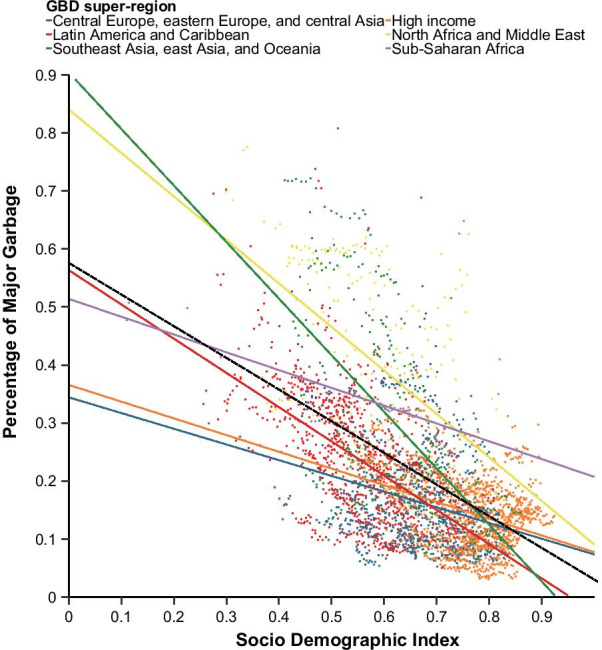
Methods: We describe the methods developed for the GBD 2019 study and subsequent iterations to redistribute garbage-coded deaths in vital registration data to plausible underlying causes. These methods include analysis of multiple cause data, negative correlation, impairment, and proportional redistribution. We classify garbage codes into classes according to the level of specificity of the reported cause of death (CoD) and capture trends in the global pattern of proportion of garbage-coded deaths, disaggregated by these classes, and the relationship between this proportion and the Socio-Demographic Index. We examine the relative importance of the top four garbage codes by age and sex and demonstrate the impact of redistribution on the annual GBD CoD rankings.
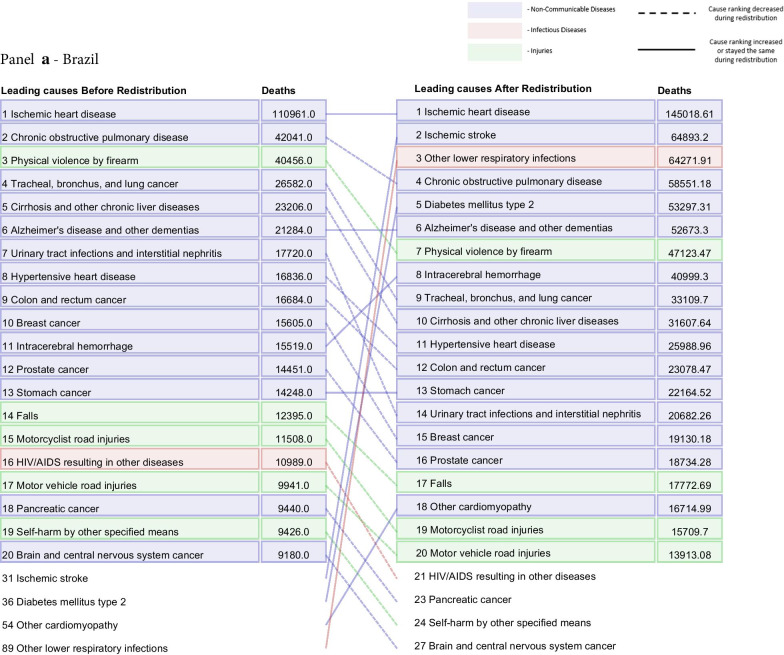
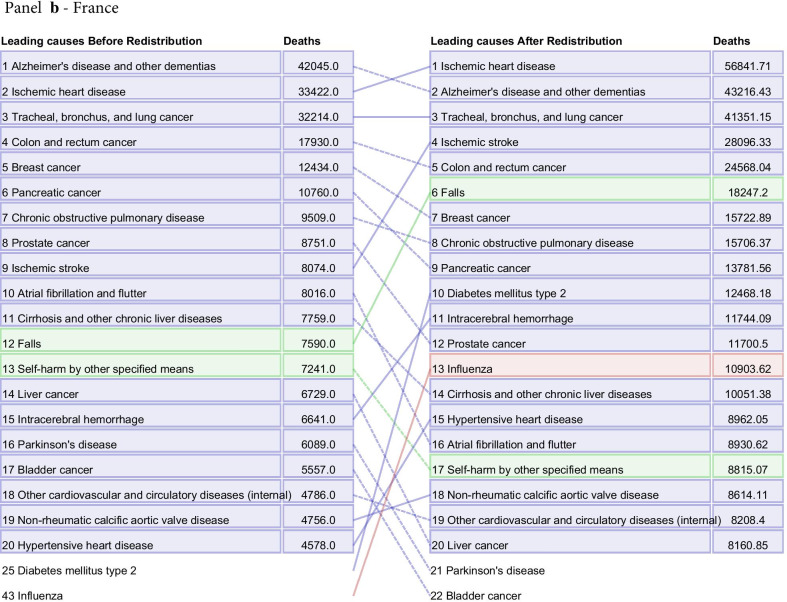
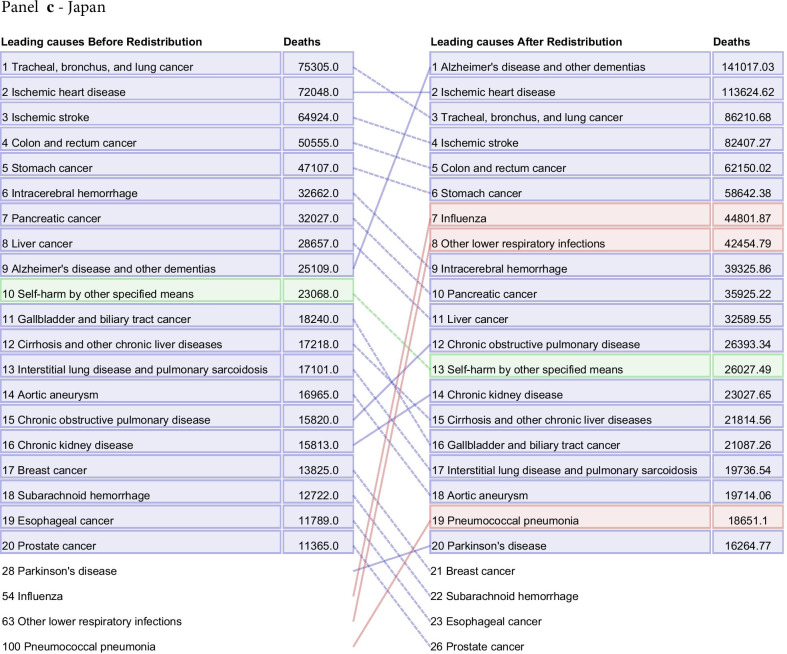
Results: The proportion of least-specific (class 1 and 2) garbage-coded deaths ranged from 3.7% of all vital registration deaths to 67.3% in 2015, and the age-standardized proportion had an overall negative association with the Socio-Demographic Index. When broken down by age and sex, the category for unspecified lower respiratory infections was responsible for nearly 30% of garbage-coded deaths in those under 1 year of age for both sexes, representing the largest proportion of garbage codes for that age group. We show how the cause distribution by number of deaths changes before and after redistribution for four countries: Brazil, the United States, Japan, and France, highlighting the necessity of accounting for garbage-coded deaths in the GBD.
Conclusions: We provide a detailed description of redistribution methods developed for CoD data in the GBD; these methods represent an overall improvement in empiricism compared to past reliance on a priori knowledge.
Keywords: Cause of death; Garbage codes; Global Burden of Disease; Redistribution; Star ranking system; Vital registration.
Conflict of interest statement
Dr. Singh reports personal fees from Crealta/Horizon, Medisys, Fidia, UBM LLC, Trio health, Adept Field solutions, Medscape, WebMD, Clinical Care options, Clearview healthcare partners, Putnam associates, Focus forward, Navigant consulting, Spherix, Practice Point communications, the National Institutes of Health and the American College of Rheumatology, personal fees from Simply Speaking, ownership in stock options from Amarin, Viking, Moderna, Vaxart pharmaceuticals, and Charlotte’s Web Holdings, non-financial support from FDA Arthritis Advisory Committee, non-financial support from Steering committee of OMERACT, an international organization that develops measures for clinical trials and receives arm’s length funding from 12 pharmaceutical companies, non-financial support from Veterans Affairs Rheumatology Field Advisory Committee, non-financial support from Editor and the Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis, outside the submitted work.
Figures


References
-
- Principles and Recommendations for a Vital Statistics System Revision 2 [Internet]. United Nations; 2001 [cited 2020 May 29]. https://unstats.un.org/unsd/publication/SeriesM/SeriesM_19rev2E.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
