

Point of care diagnostic of hypercoagulability and platelet function in COVID-19 induced acute respiratory distress syndrome: a retrospective observational study
- PMID: 34078393
- PMCID: PMC8170428
- DOI: 10.1186/s12959-021-00293-8
Point of care diagnostic of hypercoagulability and platelet function in COVID-19 induced acute respiratory distress syndrome: a retrospective observational study
Abstract
Background: Coronavirus disease 2019 (COVID-19) associated coagulopathy (CAC) leads to thromboembolic events in a high number of critically ill COVID-19 patients. However, specific diagnostic or therapeutic algorithms for CAC have not been established. In the current study, we analyzed coagulation abnormalities with point-of-care testing (POCT) and their relation to hemostatic complications in patients suffering from COVID-19 induced Acute Respiratory Distress Syndrome (ARDS). Our hypothesis was that specific diagnostic patterns can be identified in patients with COVID-19 induced ARDS at risk of thromboembolic complications utilizing POCT.
Methods: This is a single-center, retrospective observational study. Longitudinal data from 247 rotational thromboelastometries (Rotem®) and 165 impedance aggregometries (Multiplate®) were analysed in 18 patients consecutively admitted to the ICU with a COVID-19 induced ARDS between March 12th to June 30th, 2020.
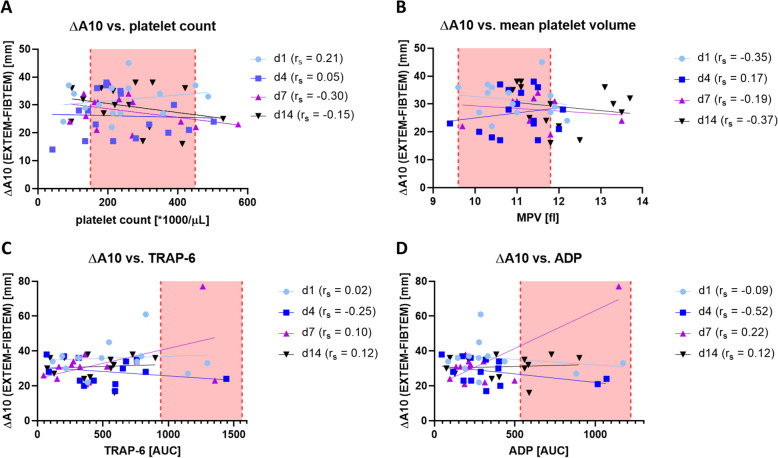
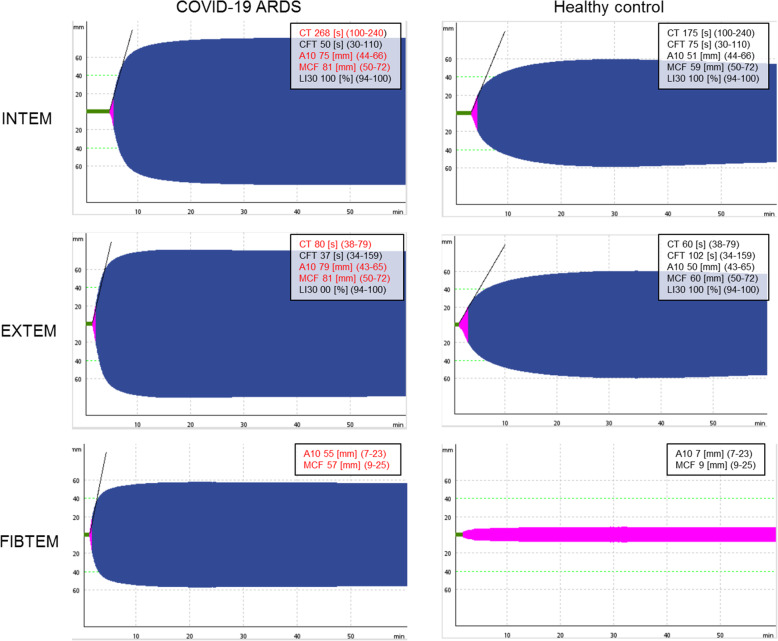
Results: Median age was 61 years (IQR: 51-69). Median PaO2/FiO2 on admission was 122 mmHg (IQR: 87-189), indicating moderate to severe ARDS. Any form of hemostatic complication occurred in 78 % of the patients with deep vein/arm thrombosis in 39 %, pulmonary embolism in 22 %, and major bleeding in 17 %. In Rotem® elevated A10 and maximum clot firmness (MCF) indicated higher clot strength. The delta between EXTEM A10 minus FIBTEM A10 (ΔA10) > 30 mm, depicting the sole platelet-part of clot firmness, was associated with a higher risk of thromboembolic events (OD: 3.7; 95 %CI 1.3-10.3; p = 0.02). Multiplate® aggregometry showed hypoactive platelet function. There was no correlation between single Rotem® and Multiplate® parameters at intensive care unit (ICU) admission and thromboembolic or bleeding complications.
Conclusions: Rotem® and Multiplate® results indicate hypercoagulability and hypoactive platelet dysfunction in COVID-19 induced ARDS but were all in all poorly related to hemostatic complications..
Keywords: Acute Respiratory Distress Syndrome; COVID-19; Impedance aggregometry; Point of care testing; Thromboelastometry.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Serial EXTEM, FIBTEM, and tPA Rotational Thromboelastometry Observations in the Maastricht Intensive Care COVID Cohort-Persistence of Hypercoagulability and Hypofibrinolysis Despite Anticoagulation.Front Cardiovasc Med. 2021 Apr 26;8:654174. doi: 10.3389/fcvm.2021.654174. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33981736 Free PMC article.
-
Prospective observational study of hemostatic alterations during adult extracorporeal membrane oxygenation (ECMO) using point-of-care thromboelastometry and platelet aggregometry.J Cardiothorac Vasc Anesth. 2015 Apr;29(2):288-96. doi: 10.1053/j.jvca.2014.06.006. Epub 2015 Feb 2. J Cardiothorac Vasc Anesth. 2015. PMID: 25655210
-
Hypercoagulability detected by whole blood thromboelastometry (ROTEM®) and impedance aggregometry (MULTIPLATE®) in obese patients.Thromb Res. 2015 Mar;135(3):548-53. doi: 10.1016/j.thromres.2015.01.003. Epub 2015 Jan 7. Thromb Res. 2015. PMID: 25592651
-
Coagulative Disorders in Critically Ill COVID-19 Patients with Acute Distress Respiratory Syndrome: A Critical Review.J Clin Med. 2021 Jan 3;10(1):140. doi: 10.3390/jcm10010140. J Clin Med. 2021. PMID: 33401632 Free PMC article. Review.
-
The Composition and Physical Properties of Clots in COVID-19 Pathology.Diagnostics (Basel). 2022 Feb 24;12(3):580. doi: 10.3390/diagnostics12030580. Diagnostics (Basel). 2022. PMID: 35328132 Free PMC article. Review.
Cited by
-
Thromboelastometry Predicts Thromboembolic Events, Hospital Length of Stay, and Mortality in Patients with COVID-19 Infection and Mild Hypoxemia: A Prospective Observational Study.J Blood Med. 2022 Jun 28;13:363-372. doi: 10.2147/JBM.S363999. eCollection 2022. J Blood Med. 2022. PMID: 35789896 Free PMC article.
-
The Role of the Kinin System and the Effect of Des-Arginine9-Bradykinin on Coagulation and Platelet Function in Critically Ill COVID-19 Patients: A Secondary Analysis of a Prospective Observational Study.Int J Mol Sci. 2024 Feb 16;25(4):2342. doi: 10.3390/ijms25042342. Int J Mol Sci. 2024. PMID: 38397016 Free PMC article.
-
Variant-derived SARS-CoV-2 spike protein does not directly cause platelet activation or hypercoagulability.Clin Exp Med. 2023 Nov;23(7):3701-3708. doi: 10.1007/s10238-023-01091-4. Epub 2023 May 19. Clin Exp Med. 2023. PMID: 37208552 Free PMC article.
-
Platelet Count in Patients with SARS-CoV-2 Infection: A Prognostic Factor in COVID-19.J Clin Med. 2022 Jul 15;11(14):4112. doi: 10.3390/jcm11144112. J Clin Med. 2022. PMID: 35887877 Free PMC article.
-
Disease Severity in Moderate-to-Severe COVID-19 Is Associated With Platelet Hyperreactivity and Innate Immune Activation.Front Immunol. 2022 Mar 11;13:844701. doi: 10.3389/fimmu.2022.844701. eCollection 2022. Front Immunol. 2022. PMID: 35359931 Free PMC article.
References
LinkOut - more resources
Full Text Sources
