

Outcome after acute ischemic stroke is linked to sex-specific lesion patterns
- PMID: 34078897
- PMCID: PMC8172535
- DOI: 10.1038/s41467-021-23492-3
Outcome after acute ischemic stroke is linked to sex-specific lesion patterns
Abstract
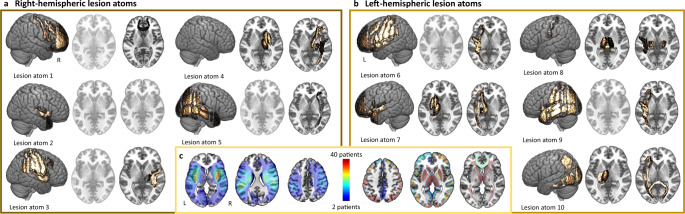
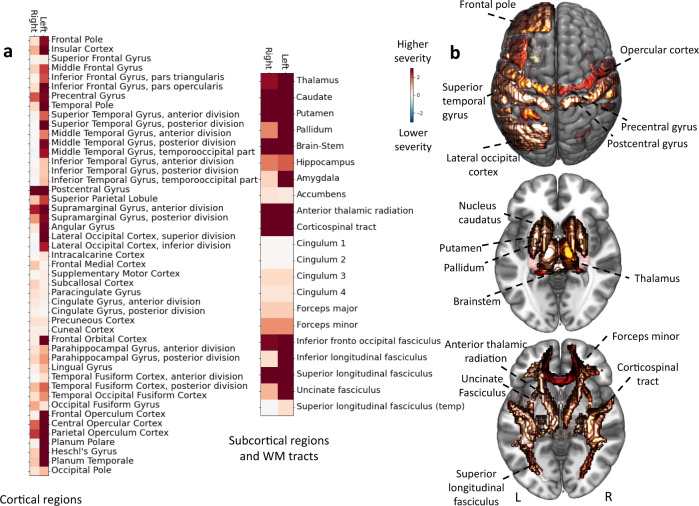
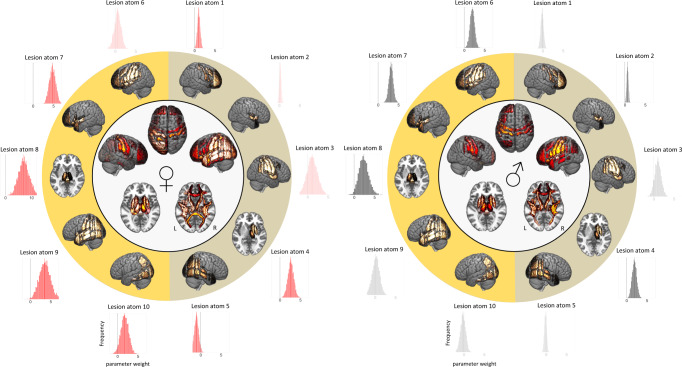
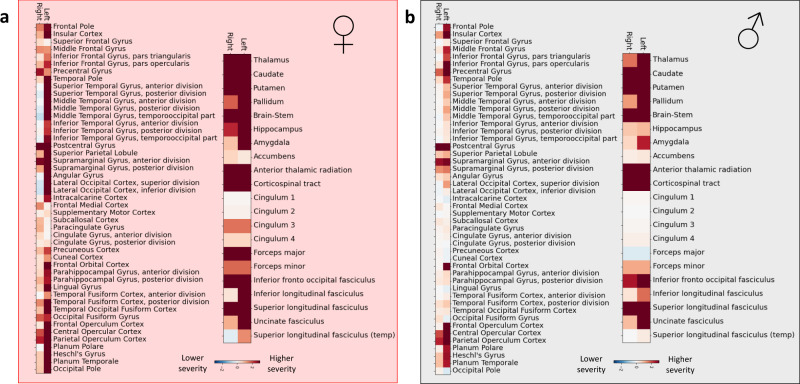
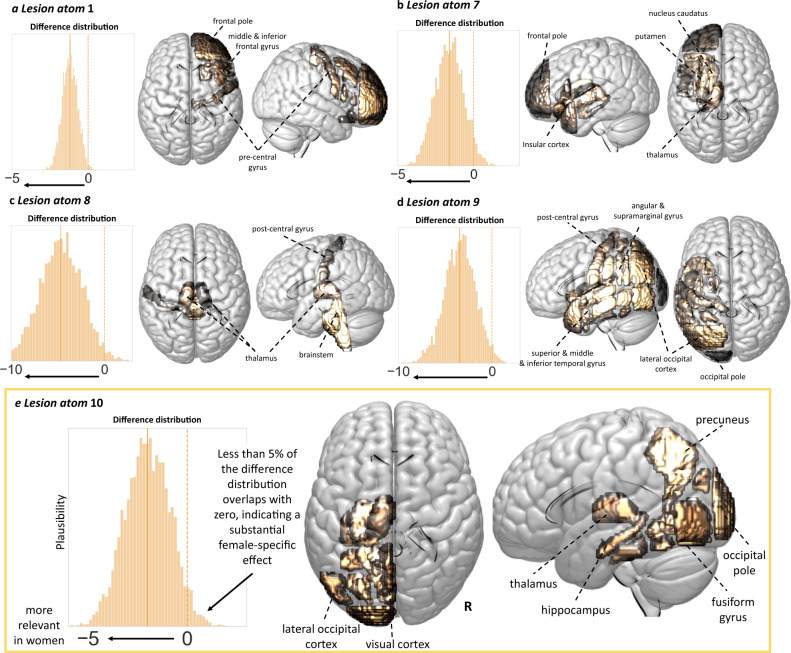
Acute ischemic stroke affects men and women differently. In particular, women are often reported to experience higher acute stroke severity than men. We derived a low-dimensional representation of anatomical stroke lesions and designed a Bayesian hierarchical modeling framework tailored to estimate possible sex differences in lesion patterns linked to acute stroke severity (National Institute of Health Stroke Scale). This framework was developed in 555 patients (38% female). Findings were validated in an independent cohort (n = 503, 41% female). Here, we show brain lesions in regions subserving motor and language functions help explain stroke severity in both men and women, however more widespread lesion patterns are relevant in female patients. Higher stroke severity in women, but not men, is associated with left hemisphere lesions in the vicinity of the posterior circulation. Our results suggest there are sex-specific functional cerebral asymmetries that may be important for future investigations of sex-stratified approaches to management of acute ischemic stroke.
Conflict of interest statement
M.E. has received personal fees for consulting from Astra Zeneca and WorldCare Clinical Group. C.G. has received consulting honoraria from Microvention and Strykere, and research funding from Medtronic and Penumbra. A.V. has received research funding from Cerenovus. A.G.L. has received personal fees from Bayer, Astra Zeneca, BMS Pfizer, and Portola. N.S.R. has received compensation as scientific advisory consultant from Omniox, Sanofi Genzyme, and AbbVie Inc. All other authors declare no competing interests.
Figures
Similar articles
-
Association of Infarct Topography and Outcome After Endovascular Thrombectomy in Patients With Acute Ischemic Stroke.Neurology. 2022 Mar 15;98(11):e1094-e1103. doi: 10.1212/WNL.0000000000200034. Epub 2022 Jan 31. Neurology. 2022. PMID: 35101908 Free PMC article.
-
Association of Stroke Lesion Pattern and White Matter Hyperintensity Burden With Stroke Severity and Outcome.Neurology. 2022 Sep 27;99(13):e1364-e1379. doi: 10.1212/WNL.0000000000200926. Epub 2022 Jul 8. Neurology. 2022. PMID: 35803717 Free PMC article.
-
The relevance of rich club regions for functional outcome post-stroke is enhanced in women.Hum Brain Mapp. 2023 Mar;44(4):1579-1592. doi: 10.1002/hbm.26159. Epub 2022 Nov 28. Hum Brain Mapp. 2023. PMID: 36440953 Free PMC article. Clinical Trial.
-
Effect of Sex on Clinical Outcome and Imaging after Endovascular Treatment of Large-Vessel Ischemic Stroke.J Stroke Cerebrovasc Dis. 2021 Feb;30(2):105468. doi: 10.1016/j.jstrokecerebrovasdis.2020.105468. Epub 2020 Nov 21. J Stroke Cerebrovasc Dis. 2021. PMID: 33227604 Free PMC article.
-
Abnormal dynamic functional connectivity is linked to recovery after acute ischemic stroke.Hum Brain Mapp. 2021 May;42(7):2278-2291. doi: 10.1002/hbm.25366. Epub 2021 Mar 2. Hum Brain Mapp. 2021. PMID: 33650754 Free PMC article.
Cited by
-
Ischemic post-conditioning is neuroprotective even at delayed tPA administration after embolic stroke in female rats.Iran J Basic Med Sci. 2021 Dec;24(12):1676-1682. doi: 10.22038/IJBMS.2021.55674.12456. Iran J Basic Med Sci. 2021. PMID: 35432799 Free PMC article.
-
The role of contralesional regions for post-stroke movements revealed by dynamic connectivity and TMS interference.Neuroimage Clin. 2025 Jun 11;47:103825. doi: 10.1016/j.nicl.2025.103825. Online ahead of print. Neuroimage Clin. 2025. PMID: 40543322 Free PMC article.
-
Research hotspots and frontiers of preconditioning in cerebral ischemia: A bibliometric analysis.Heliyon. 2024 Jan 21;10(3):e24757. doi: 10.1016/j.heliyon.2024.e24757. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38317957 Free PMC article. Review.
-
Association of Infarct Topography and Outcome After Endovascular Thrombectomy in Patients With Acute Ischemic Stroke.Neurology. 2022 Mar 15;98(11):e1094-e1103. doi: 10.1212/WNL.0000000000200034. Epub 2022 Jan 31. Neurology. 2022. PMID: 35101908 Free PMC article.
-
White matter tract correlations with spoken language in cerebrovascular disease.Brain Commun. 2025 Apr 19;7(3):fcaf145. doi: 10.1093/braincomms/fcaf145. eCollection 2025. Brain Commun. 2025. PMID: 40351387 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
