

ERCP improves mortality in acute biliary pancreatitis without cholangitis
- PMID: 34079880
- PMCID: PMC8159624
- DOI: 10.1055/a-1320-0041
ERCP improves mortality in acute biliary pancreatitis without cholangitis
Abstract
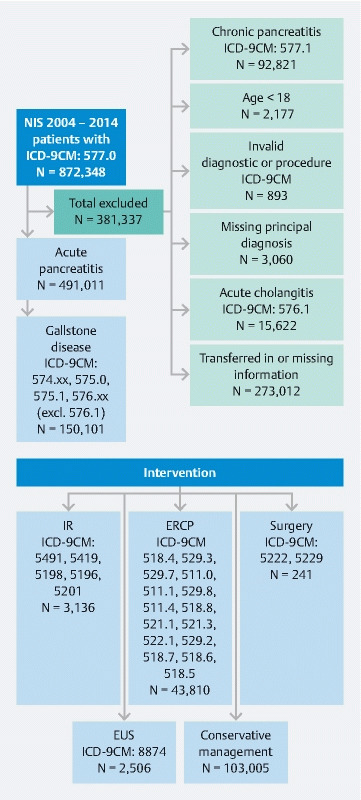
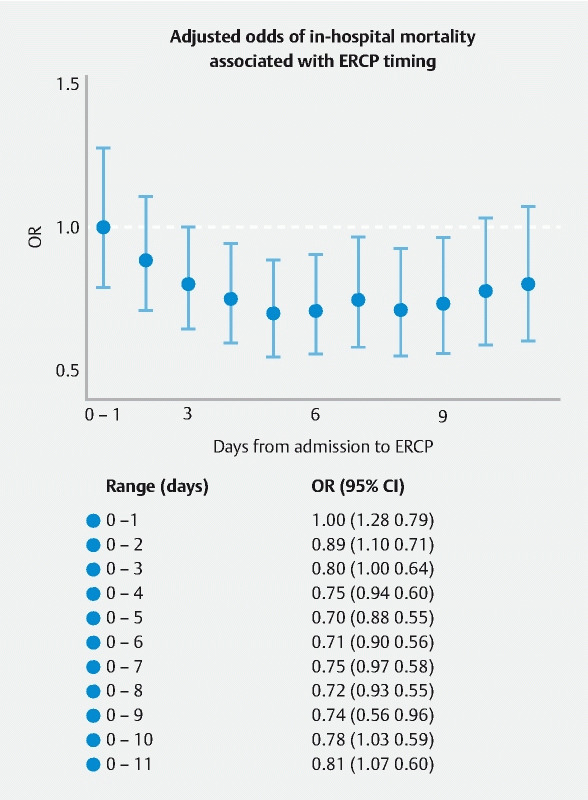
Background and study aims Acute pancreatitis (AP) is an increasingly common indication for hospitalization in the United States. The necessity for endoscopic retrograde cholangiopancreatography (ERCP) and the timing of ERCP in acute gallstone-related pancreatitis without cholangitis (AGPNC) is controversial. The aim of this study was to evaluate the association of ERCP and its performance during admission with mortality and length of stay (LOS) in patients with AGPNC. Patients and methods We queried the Nationwide Inpatient Sample (NIS) from 2004 to 2014 to identify all patients with admissions for gallstone AP. We excluded patients with chronic pancreatitis or concurrent cholangitis, and those who were transferred from elsewhere for treatment. Our primary outcome measure was inpatient mortality. Our secondary outcome measure was hospital length of stay (LOS). Results We identified 491,011 records eligible for analysis. Of the patients, 30.6 % (150,101) had AGPNC. There were 1.34 deaths per 100 admissions in patients with AGPNC. The average LOS was 5.88 (± 6.38) days with a median stay of 4 days (range, 3-7). When adjusted for age, Elixhauser Comorbidity Index, and severe pancreatitis, patients with ERCP during admission were 43 % less likely to die. ERCP performed between Days 3 and 9 of hospitalization resulted in a significant mortality benefit. Among those who had ERCP, a shorter wait time for ERCP was associated with a shorter LOS after adjustment for demographics and severity of illness. Conclusion ERCP performed during inpatient admission for AGPNC was associated with decreased mortality. These data support early ERCP in patients with acute gallstone pancreatitis without cholangitis.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
References
-
- Russo M W, Wei J T, Thiny M T et al. Digestive and liver diseases statistics, 2004. Gastroenterology. 2004;126:1448–1453. - PubMed
-
- Hirano T, Manabe T. A possible mechanism for gallstone pancreatitis: repeated short-term pancreaticobiliary duct obstruction with exocrine stimulation in rats. Proc Soc Exp Biol Med. 1993;202:246–252. - PubMed
-
- Acosta J M, Rossi R, Galli O M et al. Early surgery for acute gallstone pancreatitis: evaluation of a systematic approach. Surgery. 1978;83:367–370. - PubMed
-
- Senninger N, Moody F G, Coelho J C et al. The role of biliary obstruction in the pathogenesis of acute pancreatitis in the opossum. Surgery. 1986;99:688–693. - PubMed
LinkOut - more resources
Full Text Sources