

Comparing Renal Replacement Therapy Modalities in Critically Ill Patients With Acute Kidney Injury: A Systematic Review and Network Meta-Analysis
- PMID: 34079944
- PMCID: PMC8162503
- DOI: 10.1097/CCE.0000000000000399
Comparing Renal Replacement Therapy Modalities in Critically Ill Patients With Acute Kidney Injury: A Systematic Review and Network Meta-Analysis
Abstract
Objectives: To compare different modalities of renal replacement therapy in critically ill adults with acute kidney injury.
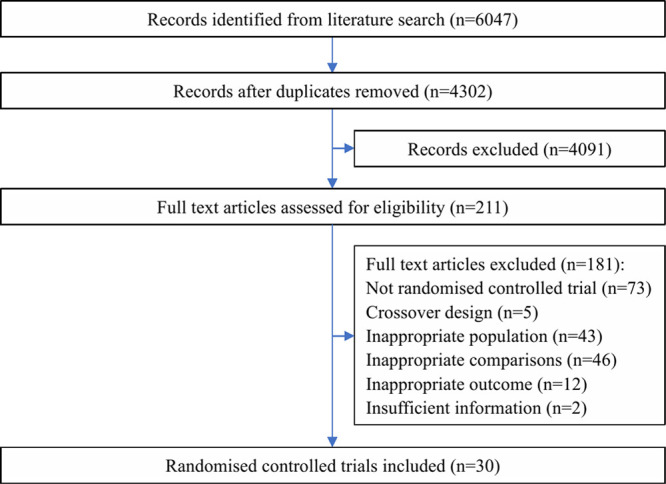
Data sources: We searched Medline, PubMed, Embase, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov from inception to 25 May, 2020. We included randomized controlled trials comparing the efficacy and safety of different renal replacement therapy modalities in critically ill patients with acute kidney injury.
Study selection: Ten reviewers (working in pairs) independently screened studies for eligibility, extracted data, and assessed risk of bias.
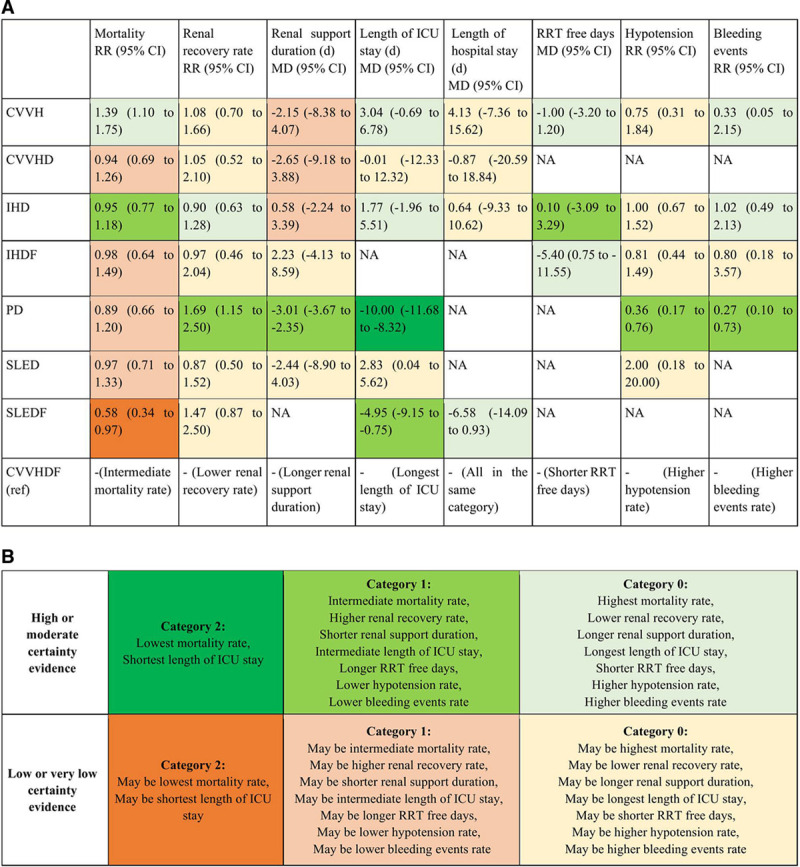
Data extraction: We performed random-effects frequentist network meta-analyses and used the Grading of Recommendations, Assessment, Development, and Evaluation approach to assess certainty of evidence. The primary analysis was a four-node analysis: continuous renal replacement therapy, intermittent hemodialysis, slow efficiency extended dialysis, and peritoneal dialysis. The secondary analysis subdivided these four nodes into nine nodes including continuous veno-venous hemofiltration, continuous veno-venous hemodialysis, continuous veno-venous hemodiafiltration, continuous arterio-venous hemodiafiltration, intermittent hemodialysis, intermittent hemodialysis with hemofiltration, slow efficiency extended dialysis, slow efficiency extended dialysis with hemofiltration, and peritoneal dialysis. We set the minimal important difference threshold for mortality as 2.5% (relative difference, 0.04).
Data synthesis: Thirty randomized controlled trials (n = 3,774 patients) proved eligible. There may be no difference in mortality between continuous renal replacement therapy and intermittent hemodialysis (relative risk, 1.04; 95% CI, 0.93-1.18; low certainty), whereas continuous renal replacement therapy demonstrated a possible increase in mortality compared with slow efficiency extended dialysis (relative risk, 1.06; 95% CI, 0.85-1.33; low certainty) and peritoneal dialysis (relative risk, 1.16; 95% CI, 0.92-1.49; low certainty). Continuous renal replacement therapy may increase renal recovery compared with intermittent hemodialysis (relative risk, 1.15; 95% CI, 0.91-1.45; low certainty), whereas both continuous renal replacement therapy and intermittent hemodialysis may be worse for renal recovery compared with slow efficiency extended dialysis and peritoneal dialysis (low certainty). Peritoneal dialysis was probably associated with the shortest duration of renal support and length of ICU stay compared with other interventions (low certainty for most comparisons). Slow efficiency extended dialysis may be associated with shortest length of hospital stay (low or moderate certainty for all comparisons) and days of mechanical ventilation (low certainty for all comparisons) compared with other interventions. There was no difference between continuous renal replacement therapy and intermittent hemodialysis in terms of hypotension (relative risk, 0.92; 95% CI, 0.72-1.16; moderate certainty) or other complications of therapy, but an increased risk of hypotension and bleeding was seen with both modalities compared with peritoneal dialysis (low or moderate certainty). Complications of slow efficiency extended dialysis were not sufficiently reported to inform comparisons.
Conclusions: The results of this network meta-analysis suggest there is no difference in mortality between continuous renal replacement therapy and intermittent hemodialysis although continuous renal replacement therapy may increases renal recovery compared with intermittent hemodialysis. Slow efficiency extended dialysis with hemofiltration may be the most effective intervention at reducing mortality. Peritoneal dialysis is associated with good efficacy, and the least number of complications however may not be practical in all settings. Importantly, all conclusions are based on very low to moderate certainty evidence, limited by imprecision. At the very least, ICU clinicians should feel comfortable that the differences between continuous renal replacement therapy, intermittent hemodialysis, slow efficiency extended dialysis, and, where clinically appropriate, peritoneal dialysis are likely small, and any of these modalities is a reasonable option to employ in critically ill patients.
Keywords: continuous renal replacement therapy; critically ill; intermittent hemodialysis; network meta-analysis; renal replacement therapy.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Collister reports personal fees from Akebia, outside the submitted work. Dr. Bagshaw reported grants and personal fees from Baxter, during the conduct of the study; personal fees from CNA Diagnostics, personal fees from BioPorto, outside the submitted work. Dr. Wald received grants and personal fees from Baxter. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Metnitz PG, Krenn CG, Steltzer H, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med. 2002; 30:2051–2058 - PubMed
-
- Uchino S, Kellum JA, Bellomo R, et al. ; Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA. 2005; 294:813–818 - PubMed
-
- Bagshaw SM, Wald R, Adhikari NKJ, et al. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med. 2020; 383:240–251 - PubMed
-
- Bellomo R, Cass A, Cole L, et al. Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med. 2009; 361:1627–1638 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
