

Outcome Improvement Between the First Two Waves of the Coronavirus Disease 2019 Pandemic in a Single Tertiary-Care Hospital in Belgium
- PMID: 34079951
- PMCID: PMC8162523
- DOI: 10.1097/CCE.0000000000000438
Outcome Improvement Between the First Two Waves of the Coronavirus Disease 2019 Pandemic in a Single Tertiary-Care Hospital in Belgium
Abstract
Objectives: To compare patient management and outcome during the first and second waves of the coronavirus 2019 pandemic.
Design: Single-center prospective cohort study.
Setting: Tertiary-care University Hospital.
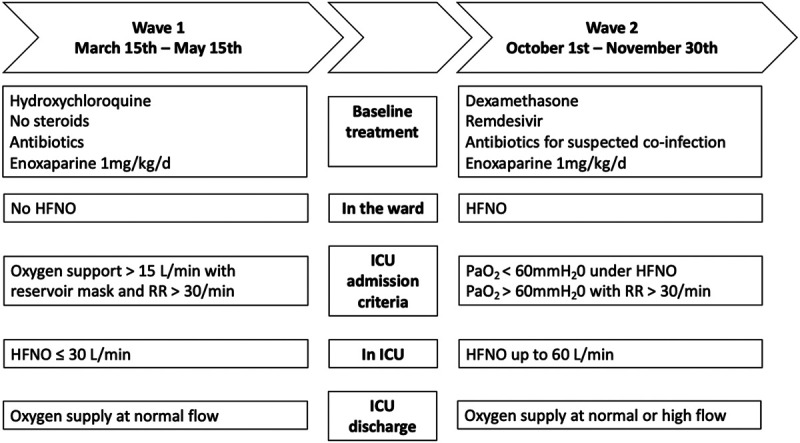
Patients: All adult patients admitted in either the first (from March 15 to May 15, 2020) or second (from October 1 to November 30, 2020) wave of coronavirus disease 2019.
Interventions: None.
Measurements and main results: Primary outcome was 30-day mortality. During the second wave of the coronavirus disease 2019 pandemic, 33 patients (4.8%) were transferred due to overcrowding and excluded from analysis. There were 341 (first wave of the coronavirus disease 2019 pandemic) and 695 (second wave of the coronavirus disease 2019 pandemic) coronavirus disease 2019 patients admitted to the hospital, with median age first wave of the coronavirus disease 2019 pandemic as 68 (57-80) and second wave of the coronavirus disease 2019 pandemic as 71 (60-80) (p = 0.15), and similar admission severity. For the first wave of the coronavirus disease 2019 pandemic versus second wave of the coronavirus disease 2019 pandemic, 30-day mortality was 74/341 (22%) and 98/662 (15%) (p = 0.007). In the ward, 11/341 (3.2%) and 404/662 (61%) received dexamethasone (p < 0.001); 6/341 (2%) and 79/662 (12%) received high-flow nasal oxygen (p < 0.0001); 2/341 (0.6%) and 88/662 (13.3%) received remdesivir (p < 0.0001); 249/341 (73%) and 0/662 (0%) received hydroxychloroquine (p < 0.0001); and 87/341 (26%) and 128/662 (19%) (p = 0.024) patients were transferred to ICU. On ICU admission, median Sequential Organ Failure Assessment was 6 (3-7) and 4 (3-6) (p = 0.02). High-flow nasal oxygen was given to 16/87 (18%) and 102/128 (80%) (p < 0.001); 69/87 (79%) and 56/128 (44%) received mechanical ventilation (p < 0.001) with durations 17 days (10-26 d) and 10 days (5-17 d) (p = 0.01). Median ICU length of stay was 14 days (5-27 d) and 6 days (3-11 d) (p < 0.001). Finally, 16/87 (18%) and 8/128 (6%) received renal replacement therapy (p = 0.0055); and 64/87 (74%) and 51/128 (40%) needed vasopressor support (p < 0.001).
Conclusions: The main therapeutic changes between the first wave of the coronavirus disease 2019 pandemic and the second wave of the coronavirus disease 2019 pandemic were use of steroids, unrestrictive use of high-flow nasal oxygen for hypoxemic patients, and transfer of patients to other geographic areas in the case of ICU overcrowding. These changes were associated with a decrease in 30-day mortality, ICU admission, and organ support.
Keywords: coronavirus disease 2019; corticosteroids; high-flow nasal oxygen; intensive care; mechanical ventilation; remdesivir.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
The Use of High-Flow Nasal Oxygen in the ICU as a First-Line Therapy for Acute Hypoxemic Respiratory Failure Secondary to Coronavirus Disease 2019.Crit Care Explor. 2020 Oct 16;2(10):e0257. doi: 10.1097/CCE.0000000000000257. eCollection 2020 Oct. Crit Care Explor. 2020. PMID: 33134947 Free PMC article.
-
Comparison of Clinical Characteristics and Outcome of Critically Ill Patients Admitted to Tertiary Care Intensive Care Units in India during the Peak Months of First and Second Waves of COVID-19 Pandemic: A Retrospective Analysis.Indian J Crit Care Med. 2021 Dec;25(12):1349-1356. doi: 10.5005/jp-journals-10071-24046. Indian J Crit Care Med. 2021. PMID: 35027793 Free PMC article.
-
Mortality comparison between the first and second/third waves among 3,795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study.Lancet Reg Health Eur. 2021 Dec;11:100243. doi: 10.1016/j.lanepe.2021.100243. Epub 2021 Nov 4. Lancet Reg Health Eur. 2021. PMID: 34751263 Free PMC article.
-
Characteristics and Outcomes of Patients With Frailty Admitted to ICU With Coronavirus Disease 2019: An Individual Patient Data Meta-Analysis.Crit Care Explor. 2022 Jan 18;4(1):e0616. doi: 10.1097/CCE.0000000000000616. eCollection 2022 Jan. Crit Care Explor. 2022. PMID: 35072081 Free PMC article. Review.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
Cited by
-
Automated evaluation of typical patient-ventilator asynchronies based on lung hysteretic responses.Biomed Eng Online. 2023 Oct 24;22(1):102. doi: 10.1186/s12938-023-01165-0. Biomed Eng Online. 2023. PMID: 37875890 Free PMC article.
-
Social health gradient and risk factors among patients hospitalized for COVID-19 and pre-pandemic respiratory infections. A linked national individual case-control study in Belgium.Front Public Health. 2024 Oct 28;12:1426898. doi: 10.3389/fpubh.2024.1426898. eCollection 2024. Front Public Health. 2024. PMID: 39529714 Free PMC article.
-
One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment.Healthcare (Basel). 2022 Oct 13;10(10):2023. doi: 10.3390/healthcare10102023. Healthcare (Basel). 2022. PMID: 36292470 Free PMC article.
-
Impact of Severity of Maternal COVID-19 Infection on Perinatal Outcome and Vertical Transmission Risk: An Ambispective Study From North India.Cureus. 2022 Feb 1;14(2):e21820. doi: 10.7759/cureus.21820. eCollection 2022 Feb. Cureus. 2022. PMID: 35261838 Free PMC article.
-
Intensive care burden of COVID-19 in tertiary care hospitals during the first year of outbreak in Kawasaki City, Japan: A retrospective cohort study.J Infect Chemother. 2022 May;28(5):678-683. doi: 10.1016/j.jiac.2022.01.022. Epub 2022 Feb 9. J Infect Chemother. 2022. PMID: 35177351 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Medical
