

SCOPE 2021: a new scorecard for osteoporosis in Europe
- PMID: 34080059
- PMCID: PMC8172408
- DOI: 10.1007/s11657-020-00871-9
SCOPE 2021: a new scorecard for osteoporosis in Europe
Abstract
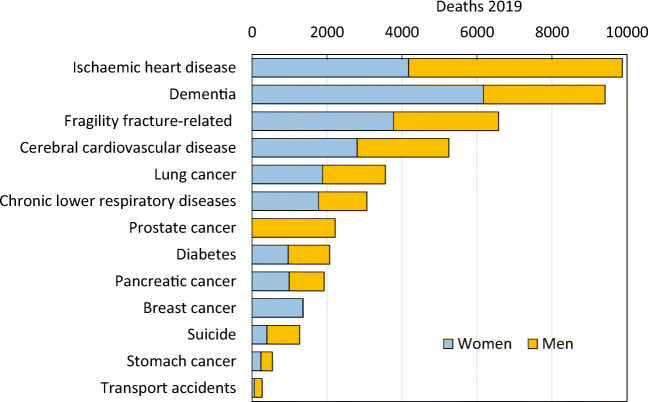
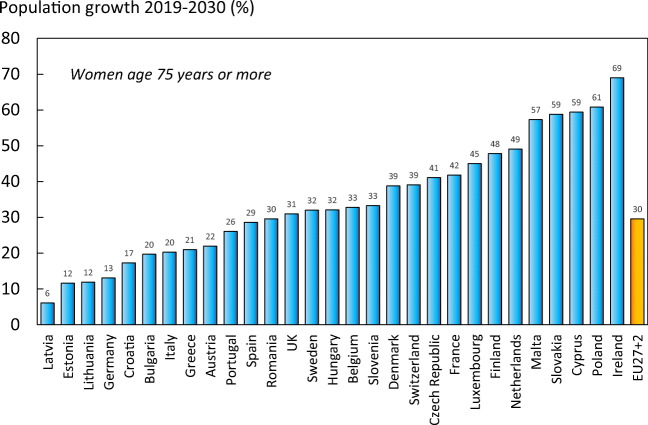
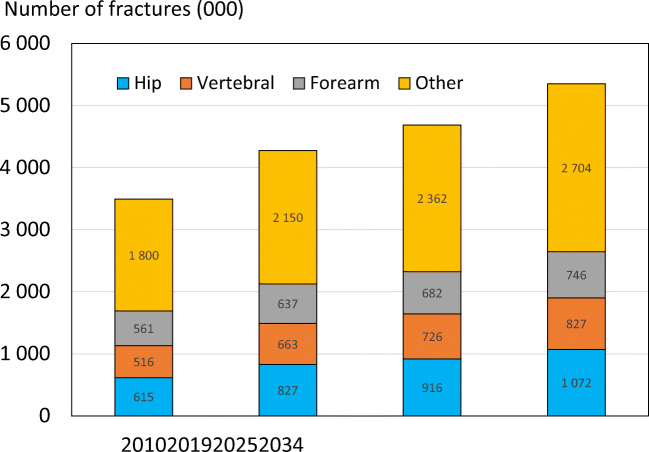
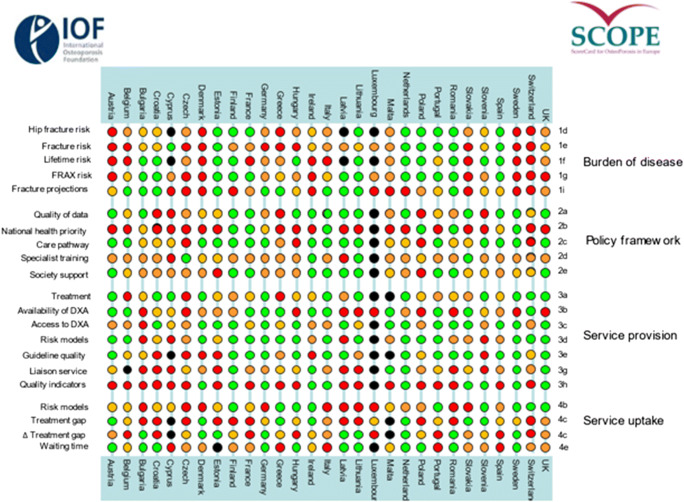
This scorecard summarises key indicators of the burden of osteoporosis and its management in the 27 member states of the European Union, as well as the UK and Switzerland. The resulting scorecard elements, assembled on a single sheet, provide a unique overview of osteoporosis in Europe.
Introduction: The scorecard for osteoporosis in Europe (SCOPE) is a project of the International Osteoporosis Foundation (IOF) that seeks to raise awareness of osteoporosis care in Europe. The aim of this project was to develop a scorecard and background documents to draw attention to gaps and inequalities in the provision of primary and secondary prevention of fractures due to osteoporosis.
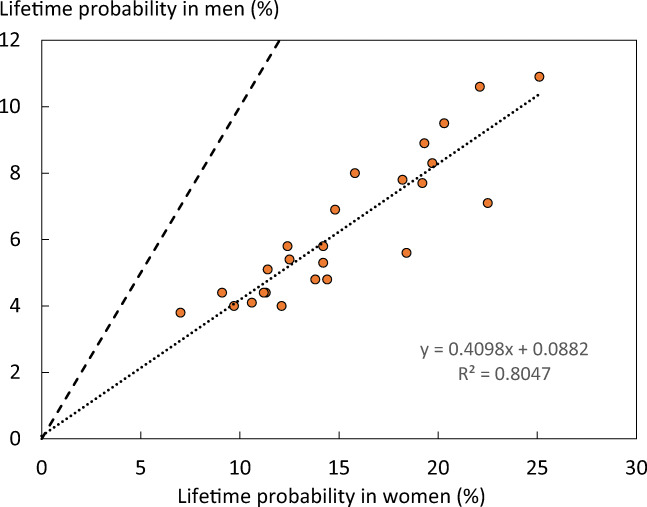
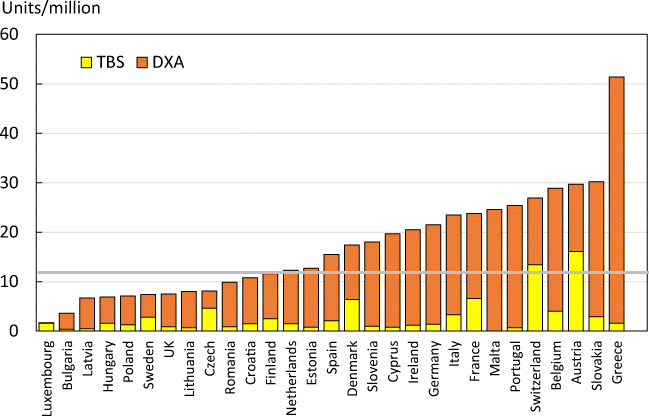
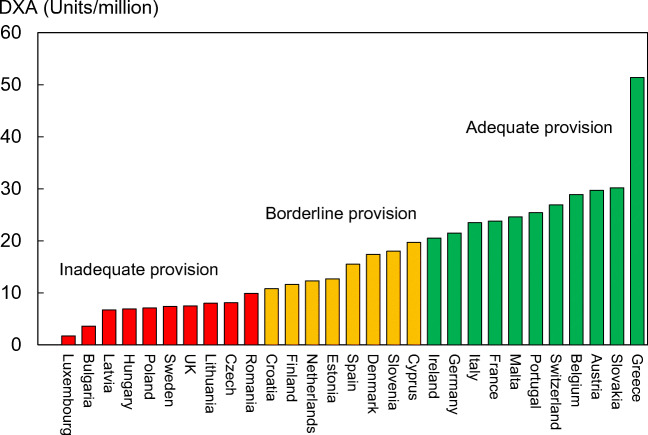
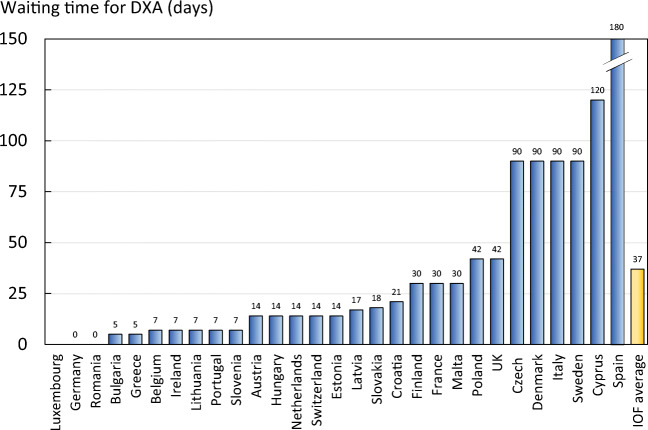
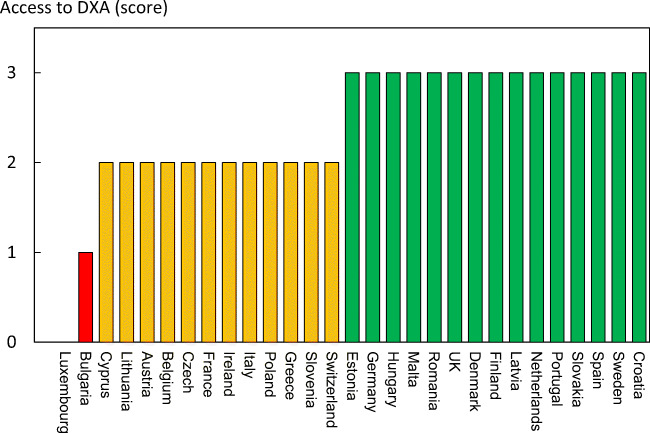
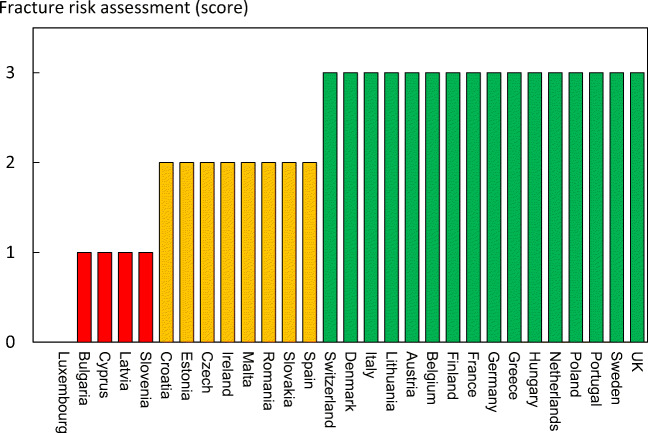
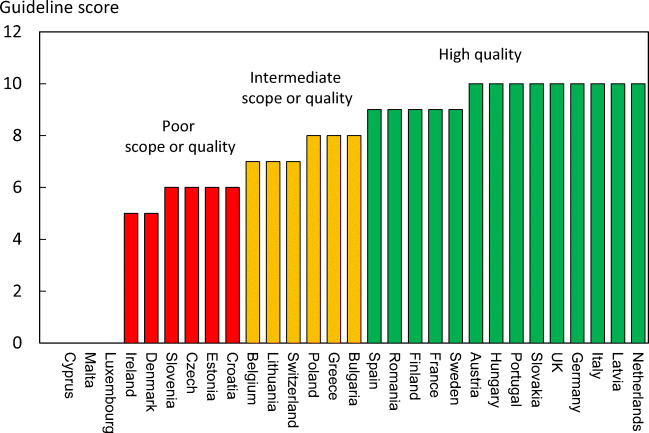
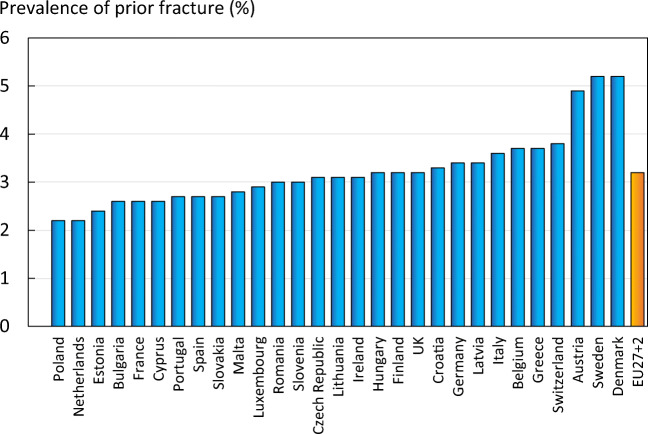
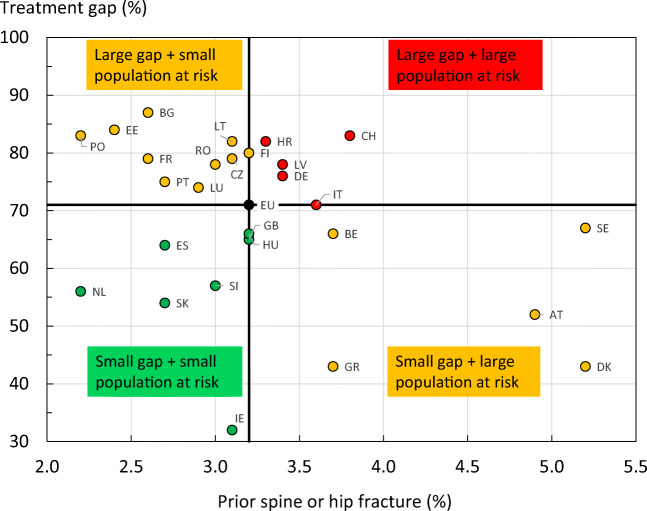
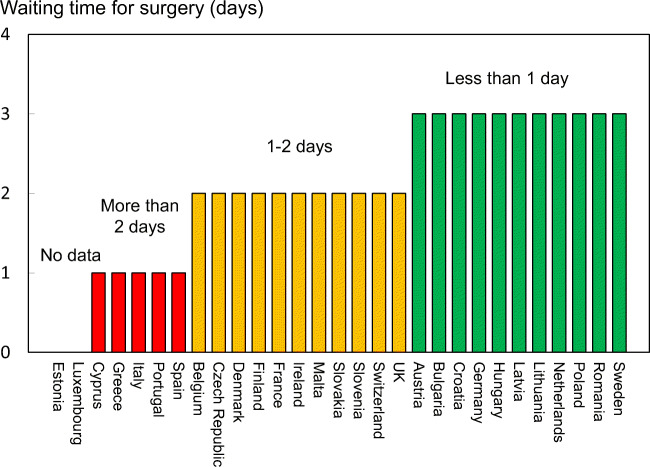
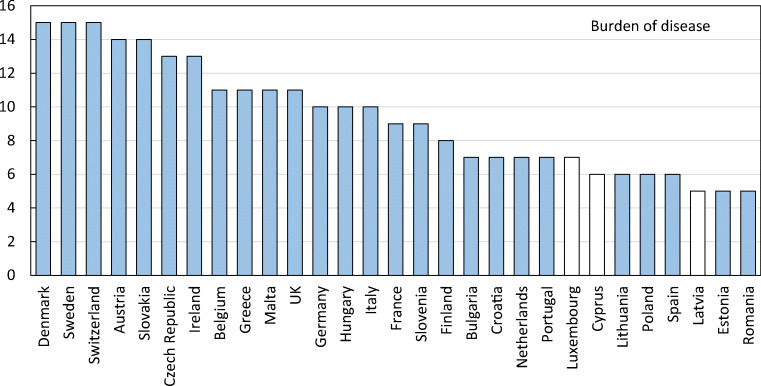
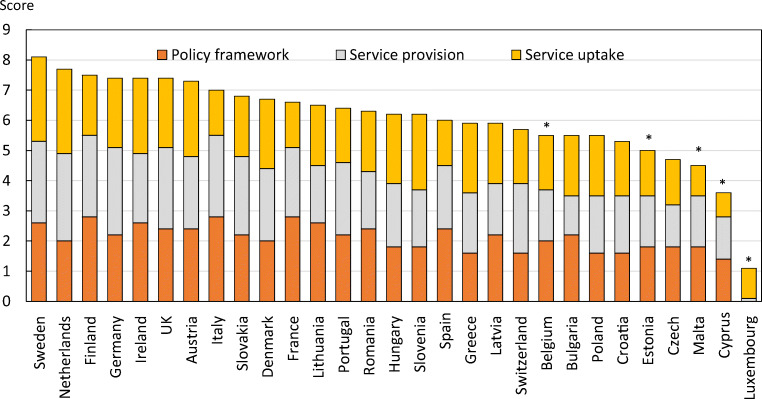
Methods: The SCOPE panel reviewed the information available on osteoporosis and the resulting fractures for each of the 27 countries of the European Union plus the UK and Switzerland (termed EU27+2). The information obtained covered four domains: background information (e.g. the burden of osteoporosis and fractures), policy framework, service provision and service uptake, e.g. the proportion of men and women at high risk that do not receive treatment (the treatment gap).
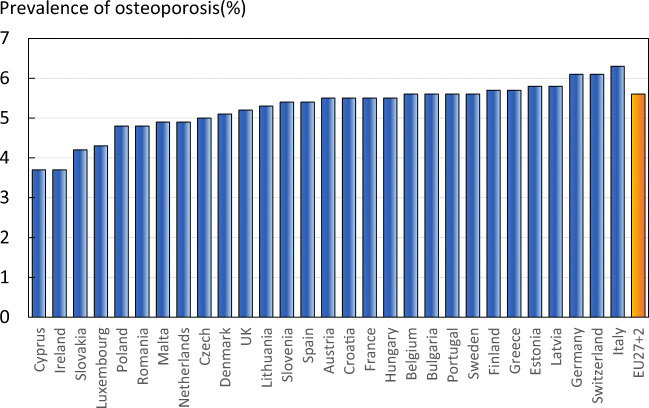
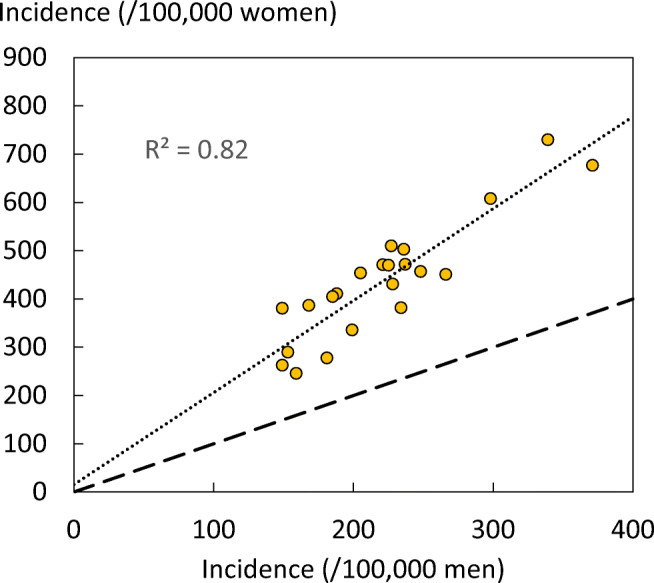
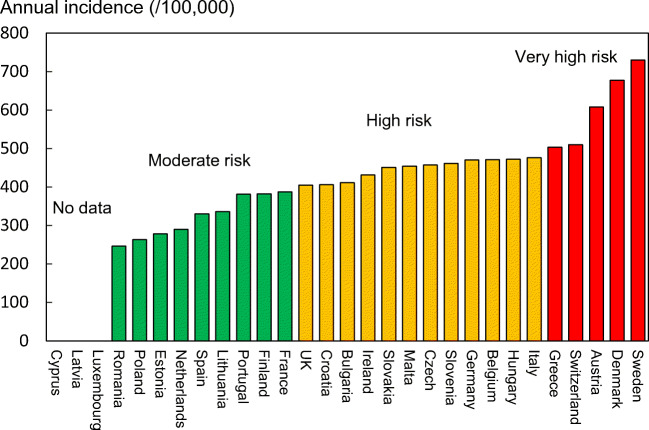
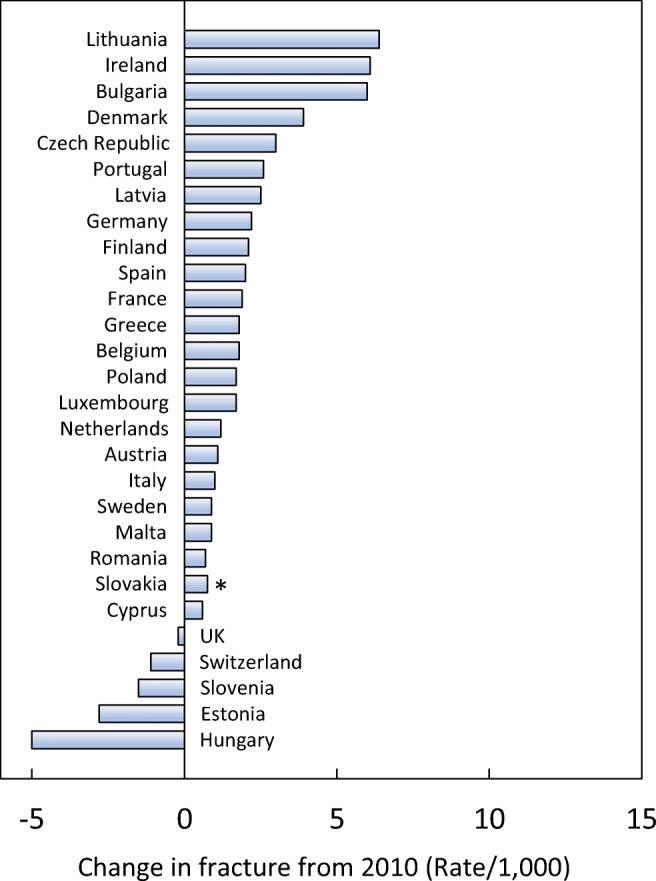
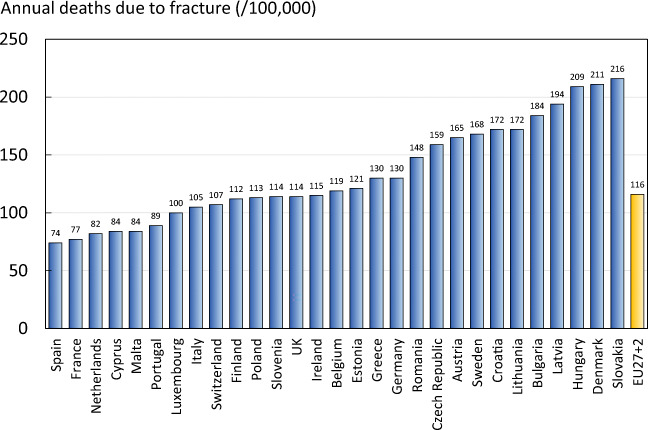
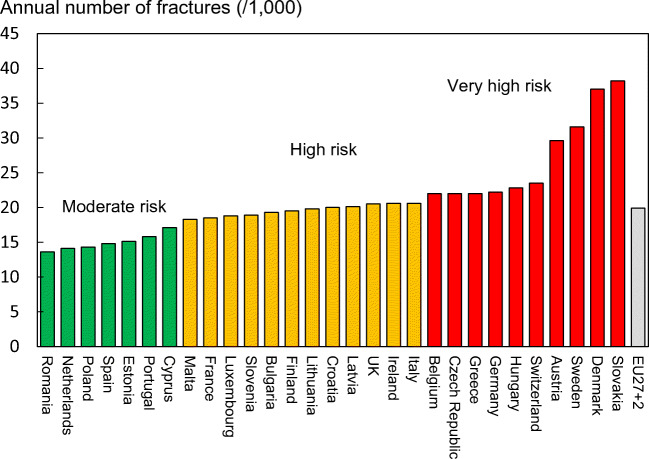
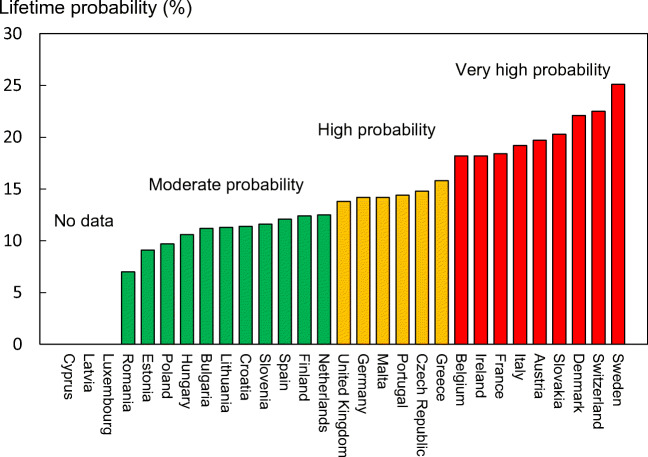
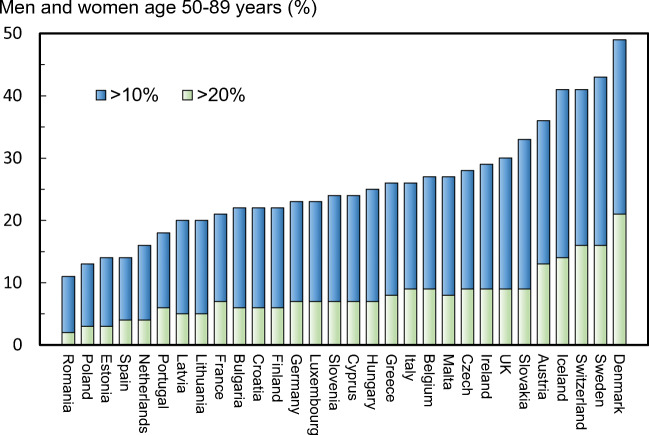
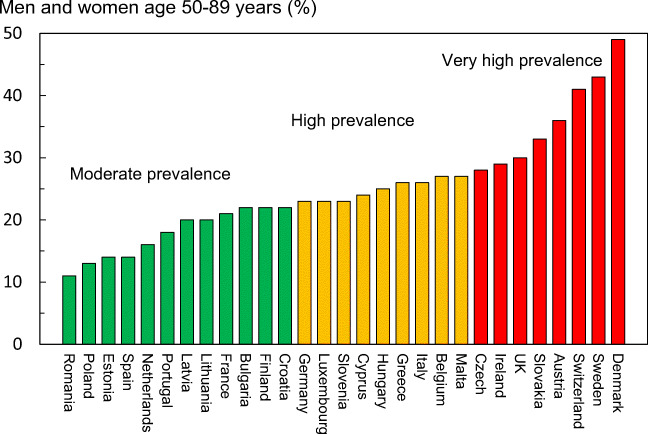
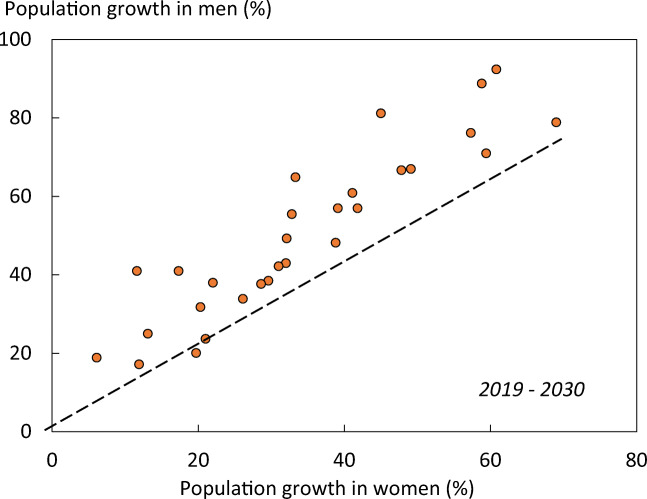
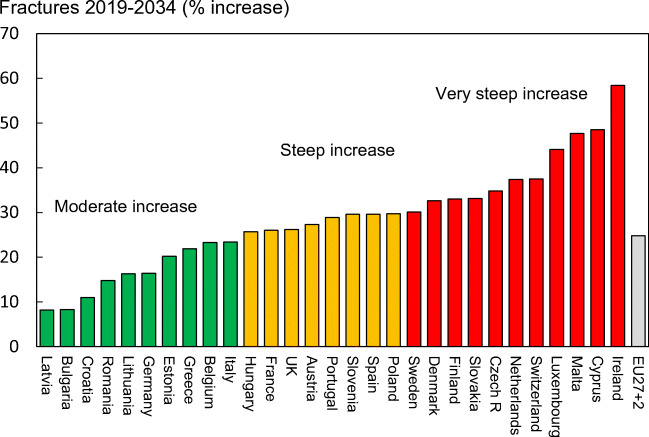
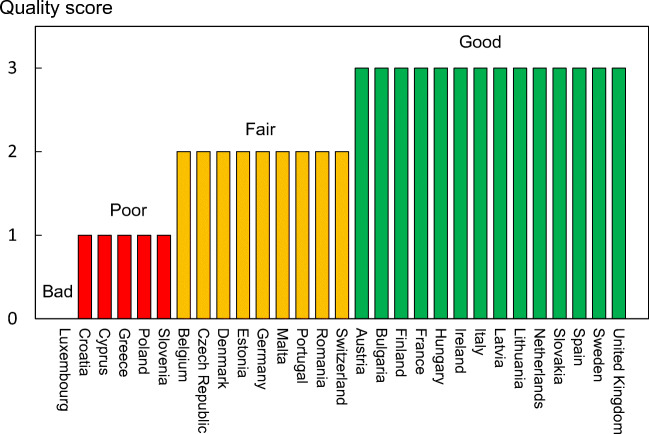
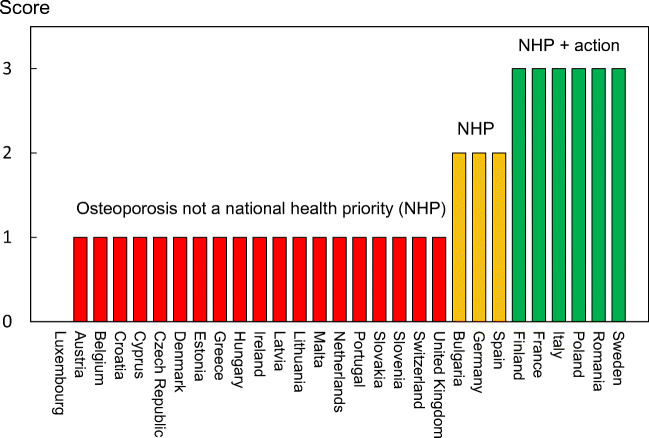
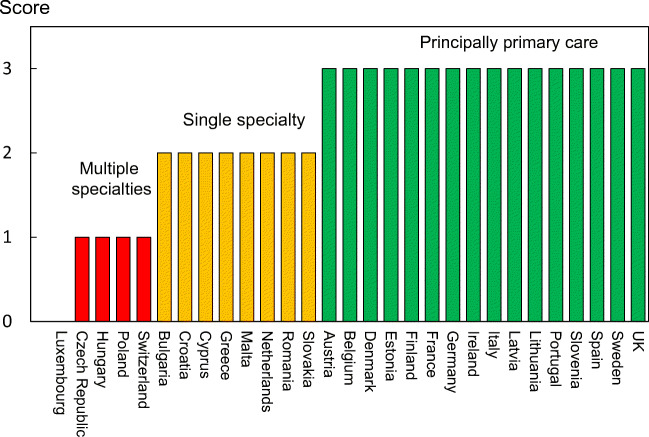
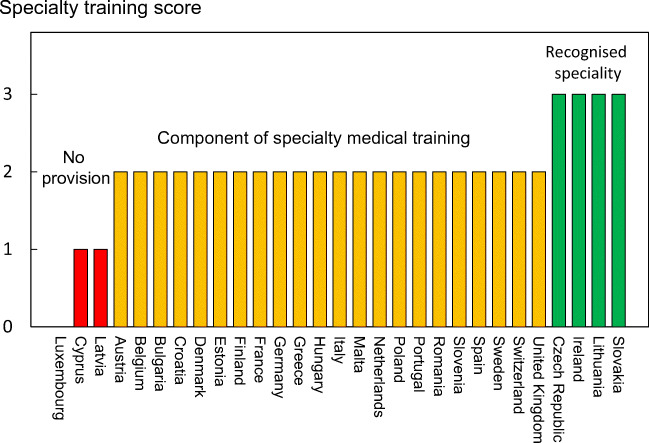
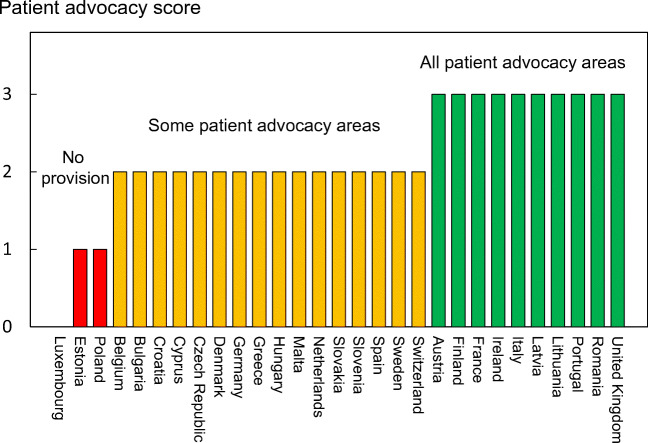
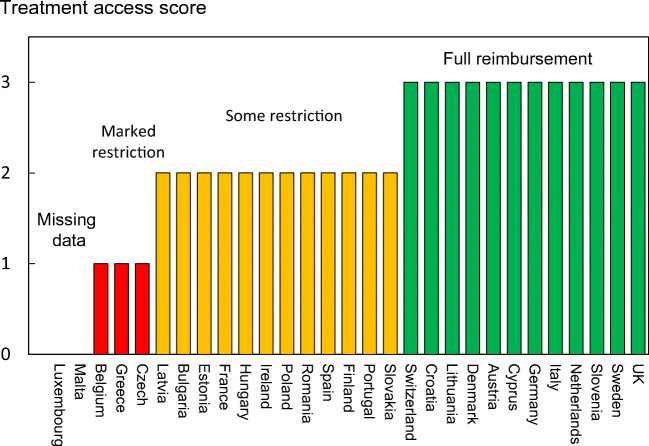
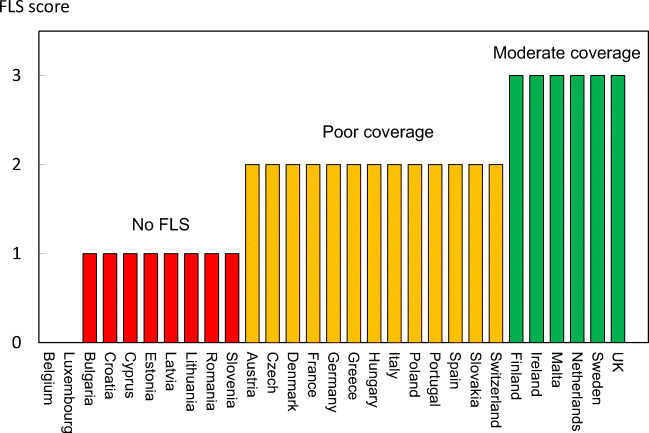
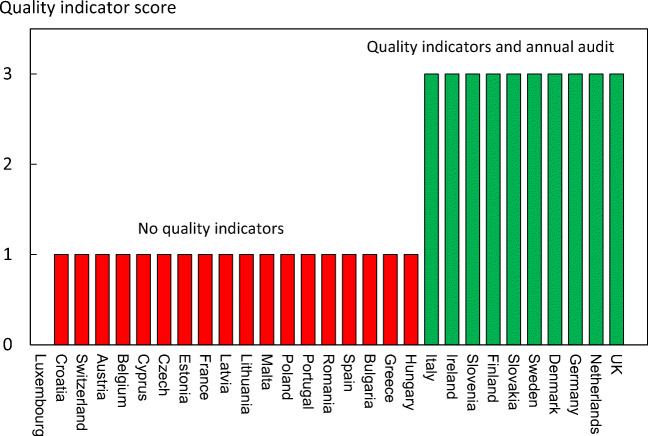
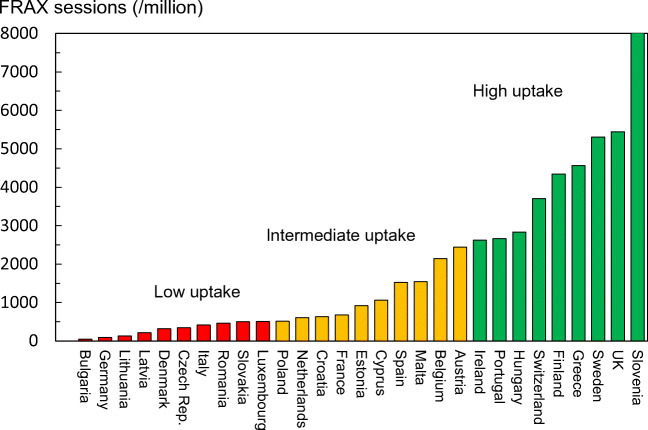
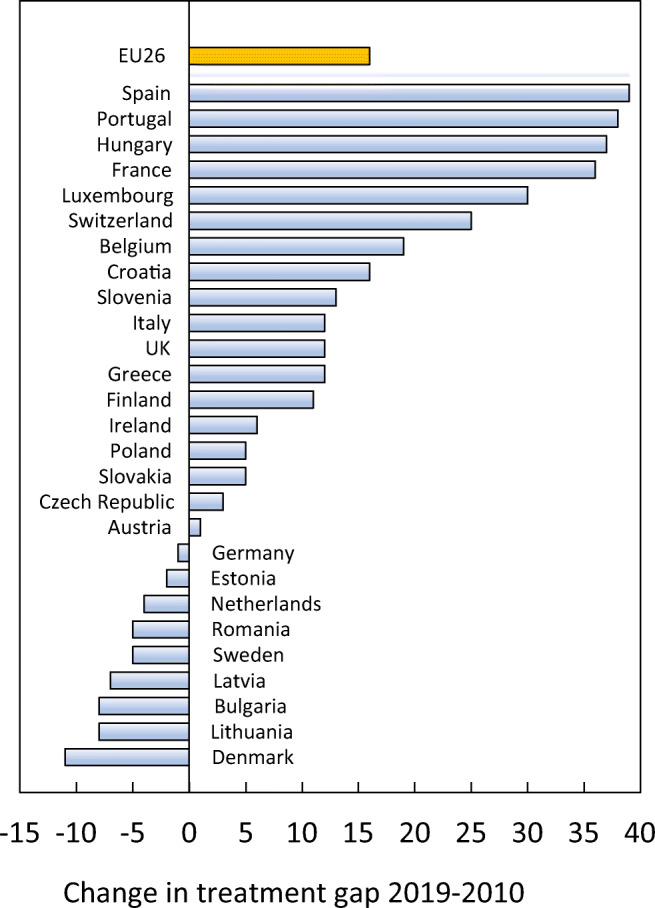
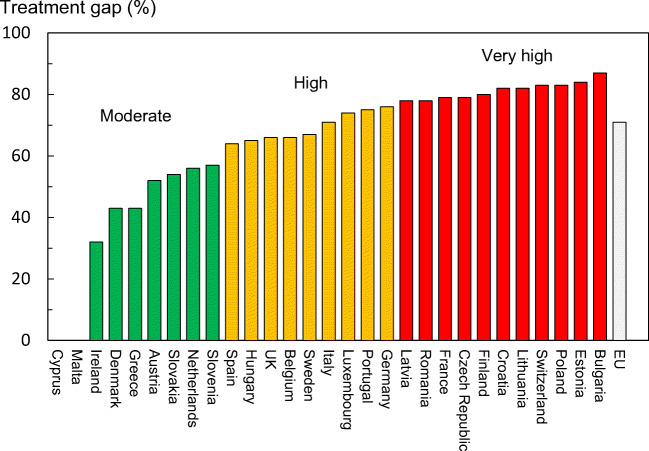
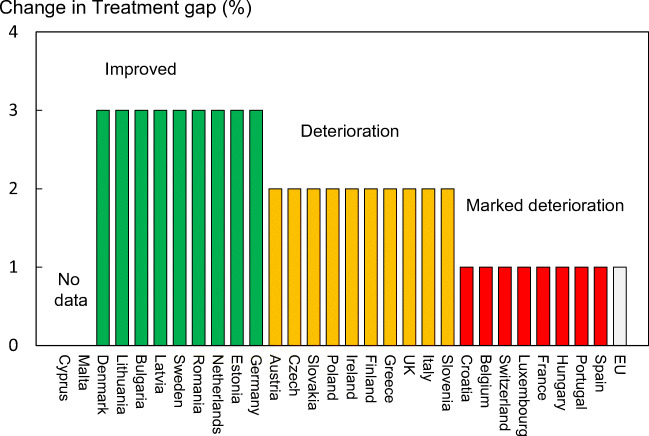
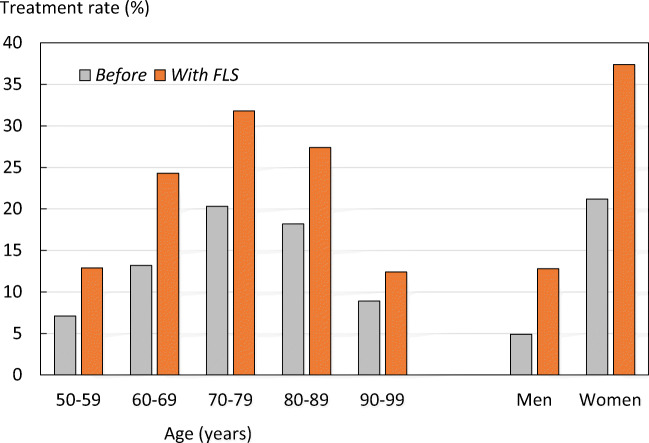
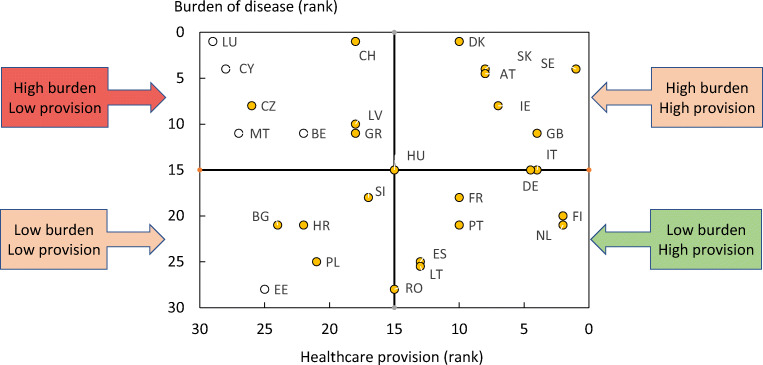
Results: There was a marked difference in fracture risk among the EU27+2 countries. Of concern was the marked heterogeneity in the policy framework, service provision and service uptake for osteoporotic fracture that bore little relation to the fracture burden. For example, despite the wide availability of treatments to prevent fractures, in the majority of the EU27+2, only a minority of patients at high risk receive treatment even after their first fracture. The elements of each domain in each country were scored and coded using a traffic light system (red, orange, green) and used to synthesise a scorecard. The resulting scorecard elements, assembled on a single sheet, provide a unique overview of osteoporosis in Europe.
Conclusions: The scorecard enables healthcare professionals and policy makers to assess their country's general approach to the disease and provide indicators to inform the future provision of healthcare.
Keywords: Burden of disease; Cost; Epidemiology; European Union; Osteoporosis; Policy framework; SCOPE; Scorecard; Service provision; Service uptake; Treatment gap; Treatment uptake.
Conflict of interest statement
F Borgström is employed and is a shareholder in Quantify Research, a health economic research consultancy that received a grant from IOF to conduct the analysis. N Norton, C Willers and T Jacobson are employed by Quantify Research, a health economic research consultancy that received a grant from IOF to conduct the analysis. N. Harvey has received consultancy, lecture fees and honoraria from Alliance for Better Bone Health, AMGEN, MSD, Eli Lilly, Servier, Shire, UCB, Kyowa Kirin, Consilient Healthcare, Radius Health and Internis Pharma. EV McCloskey has received consultancy/lecture fees/grant funding/honoraria from AgNovos, Amgen, AstraZeneca, Consilient Healthcare, Fresenius Kabi, Gilead, GSK, Hologic, Internis, Lilly, Merck, Novartis, Pfizer, Radius Health, Redx Oncology, Roche, SanofiAventis, Servier, Synexus, UCB, Viiv, Warner Chilcott, I3 Innovus and Unilever. JA Kanis is the architect of FRAX® but has no financial interest. M Lorentzon has received lecture fees from Amgen, Lilly, Meda, Renapharma, UCB Pharma, and consulting fees from Amgen, Radius Health, UCB Pharma, Renapharma and Consilient Health, all outside the presented work
Figures
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
