

Asthma phenotypes, associated comorbidities, and long-term symptoms in COVID-19
- PMID: 34080210
- PMCID: PMC8222896
- DOI: 10.1111/all.14972
Asthma phenotypes, associated comorbidities, and long-term symptoms in COVID-19
Abstract
Background: It is unclear whether asthma and its allergic phenotype are risk factors for hospitalization or severe disease from SARS-CoV-2.
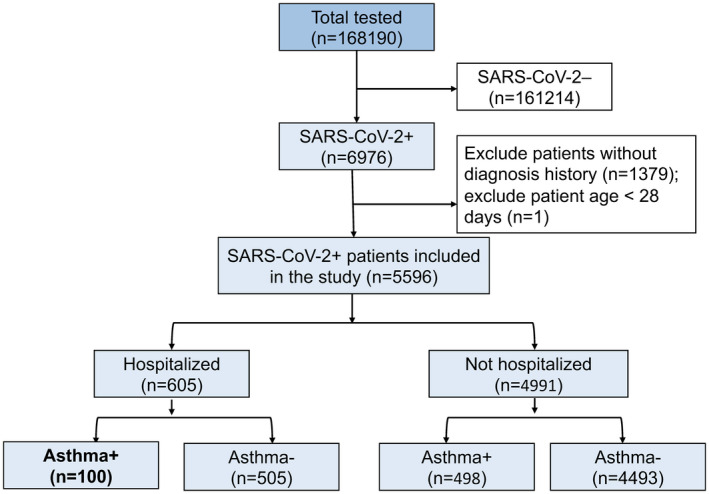
Methods: All patients over 28 days old testing positive for SARS-CoV-2 between March 1 and September 30, 2020, were retrospectively identified and characterized through electronic analysis at Stanford. A sub-cohort was followed prospectively to evaluate long-term COVID-19 symptoms.
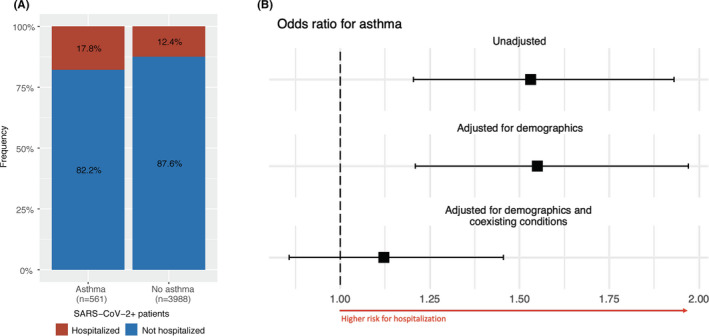
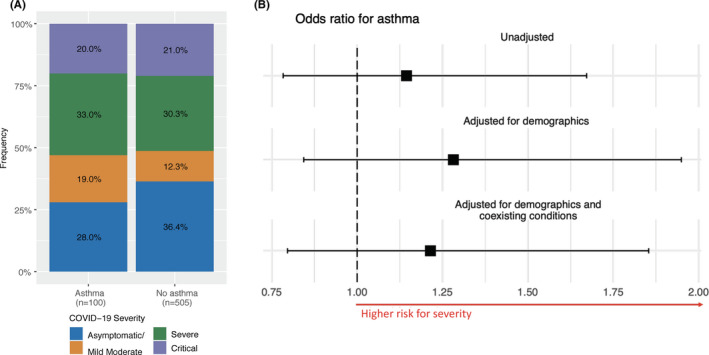
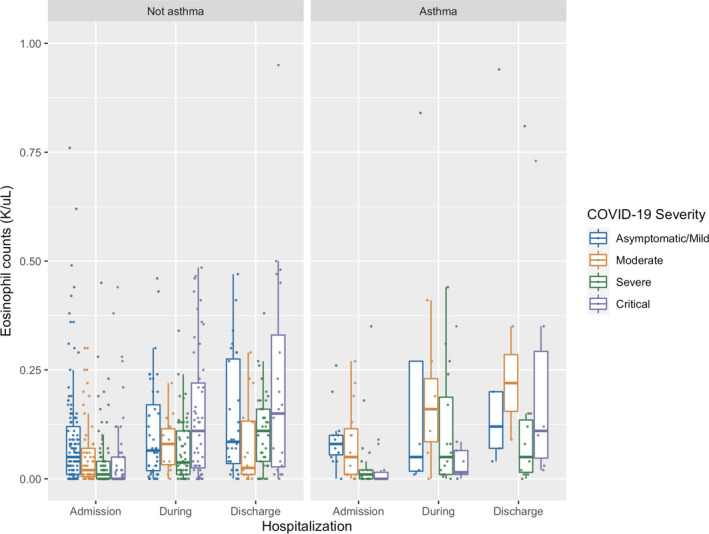
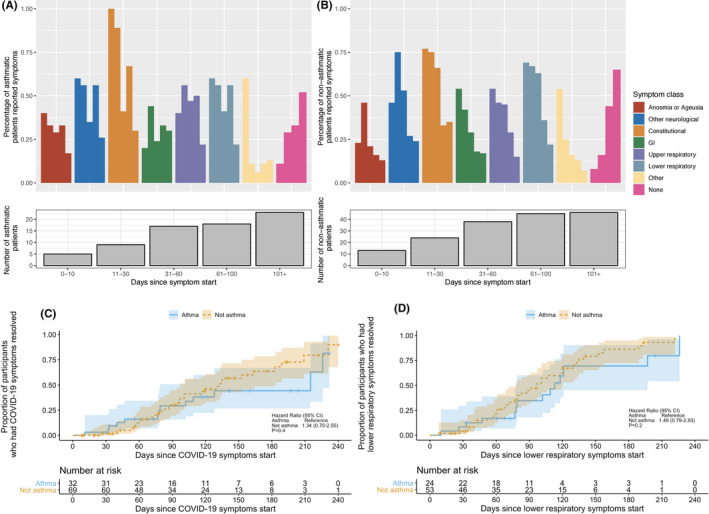
Results: 168,190 patients underwent SARS-CoV-2 testing, and 6,976 (4.15%) tested positive. In a multivariate analysis, asthma was not an independent risk factor for hospitalization (OR 1.12 [95% CI 0.86, 1.45], p = .40). Among SARS-CoV-2-positive asthmatics, allergic asthma lowered the risk of hospitalization and had a protective effect compared with non-allergic asthma (OR 0.52 [0.28, 0.91], p = .026); there was no association between baseline medication use as characterized by GINA and hospitalization risk. Patients with severe COVID-19 disease had lower eosinophil levels during hospitalization compared with patients with mild or asymptomatic disease, independent of asthma status (p = .0014). In a patient sub-cohort followed longitudinally, asthmatics and non-asthmatics had similar time to resolution of COVID-19 symptoms, particularly lower respiratory symptoms.
Conclusions: Asthma is not a risk factor for more severe COVID-19 disease. Allergic asthmatics were half as likely to be hospitalized with COVID-19 compared with non-allergic asthmatics. Lower levels of eosinophil counts (allergic biomarkers) were associated with a more severe COVID-19 disease trajectory. Recovery was similar among asthmatics and non-asthmatics with over 50% of patients reporting ongoing lower respiratory symptoms 3 months post-infection.
Keywords: COVID-19; SARS-CoV-2; asthma; eosinophils.
© 2021 European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
LE, ZH, AL, TS, JF, SC, RO, MA, LB, BP, SJ, RP, RW, AB, GD, and NA report no conflicts of interest. WC reports research support from Regeneron.MD reports receiving grant funding from the Ping Li and Kim Li Endowment and the NIH. SS reports receiving grant funding from the NIH, Regeneron, DBV Technologies, Aimmune, Novartis, and CoFAR. KN reports grant funding from NIAID, NHLBI, NIEHS, and FARE, and support from the Sunshine Foundation, Parker Foundation, and Crown Foundation.SC receives grant funding from NIAID, CoFAR, Aimmune, DBV Technologies, Astellas, Regeneron, and FARE and support from the Maternal Child Health Research Institute, Sunshine Foundation, Parker Foundation, and Crown Foundation.
Figures

Comment in
-
SARS-CoV-2 infection in severe asthma is associated with worsening of COVID-19 through respiratory NLRP3 inflammasome activation.Allergy. 2023 Jan;78(1):287-290. doi: 10.1111/all.15452. Epub 2022 Aug 5. Allergy. 2023. PMID: 35871401 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
