

Non-alcoholic fatty liver disease and sarcopenia additively increase mortality: a Korean nationwide survey
- PMID: 34080327
- PMCID: PMC8350204
- DOI: 10.1002/jcsm.12719
Non-alcoholic fatty liver disease and sarcopenia additively increase mortality: a Korean nationwide survey
Abstract
Background: Sarcopenia is an independent risk factor not only for advanced-stage non-alcoholic fatty liver disease (NAFLD) but also for mortality. We investigated the association of sarcopenia and/or NAFLD with mortality among the Korean general population.
Methods: Individuals aged 35-75 years without any history of cancer, ischaemic heart disease, ischaemic stroke, or secondary causes of chronic liver disease were selected from the Korean National Health and Nutrition Examination Surveys from 2008 to 2015. Their mortality data until December 2018 were retrieved from the National Death Registry. NAFLD and sarcopenia were defined by hepatic steatosis index and appendicular skeletal muscle mass divided by body mass index (BMI), respectively.
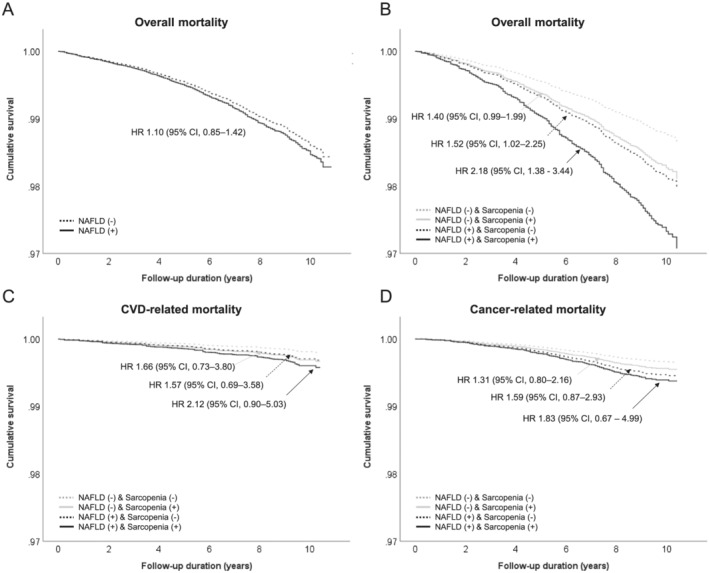
Results: A total of 28 060 subjects were analysed [mean age, 50.6 (standard error, 0.1) years, 48.2 (0.3) % men]; the median follow-up duration was of 6.8 (interquartile range, 4.8, 8.4) years. NAFLD predicted mortality after adjustment for age, sex, BMI, hypertension, dyslipidaemia, and smoking (HR 1.32, 95% CI 1.03-1.70), but this prediction lost its statistical significance after additional adjustment for diabetes mellitus. In contrast, NAFLD with advanced fibrosis independently increased the risk of mortality after adjustment for all covariates (HR 1.68, 95% CI 1.02-2.79). Stratified analysis revealed that NAFLD and sarcopenia additively increased the risk of mortality as an ordinal scale (HR 1.46, 95% CI 1.18-1.81, P for trend = 0.001). The coexistence of NAFLD and sarcopenia increased the risk of mortality by almost twice as much, even after adjustment for advanced fibrosis (HR 2.18, 95% CI 1.38-3.44).
Conclusions: Concurrent NAFLD and sarcopenia conferred a two-fold higher risk of mortality. The observation that NAFLD and sarcopenia additively increase mortality suggests that risk stratification would be helpful in predicting mortality among those with metabolic derangement.
Keywords: Mortality; Nationwide survey; Non-alcoholic fatty liver disease; Sarcopenia.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, Contreras M, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle‐aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124–131. - PubMed
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018;15:11–20. - PubMed
-
- Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non‐alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta‐analysis. J Hepatol 2016;65:589–600. - PubMed
-
- Torres DM, Williams CD, Harrison SA. Features, diagnosis, and treatment of nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2012;10:837–858. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
