Role of Computed Tomography in Pre- and Postoperative Evaluation of a Double-Outlet Right Ventricle
- PMID: 34080329
- PMCID: PMC8318812
- DOI: 10.4250/jcvi.2020.0196
Role of Computed Tomography in Pre- and Postoperative Evaluation of a Double-Outlet Right Ventricle
Abstract
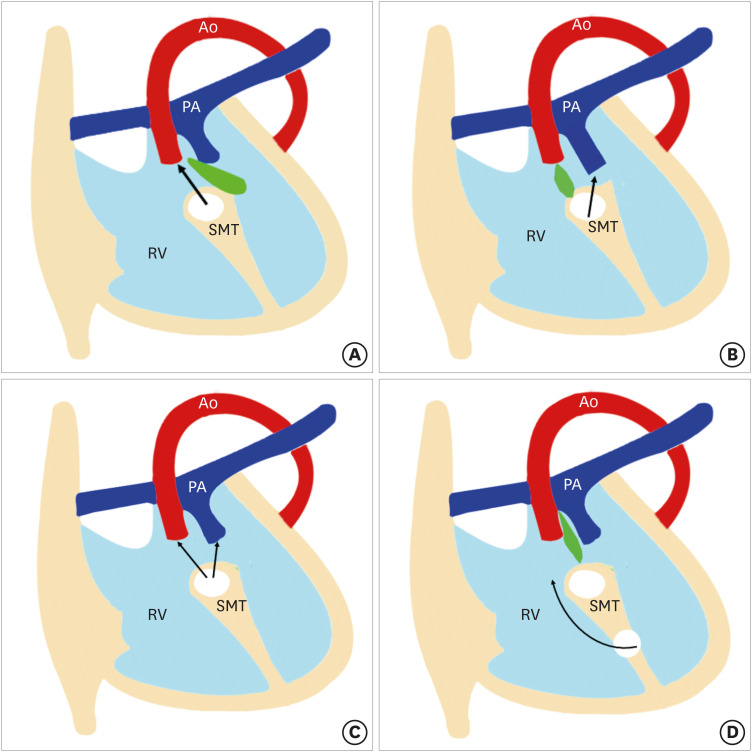
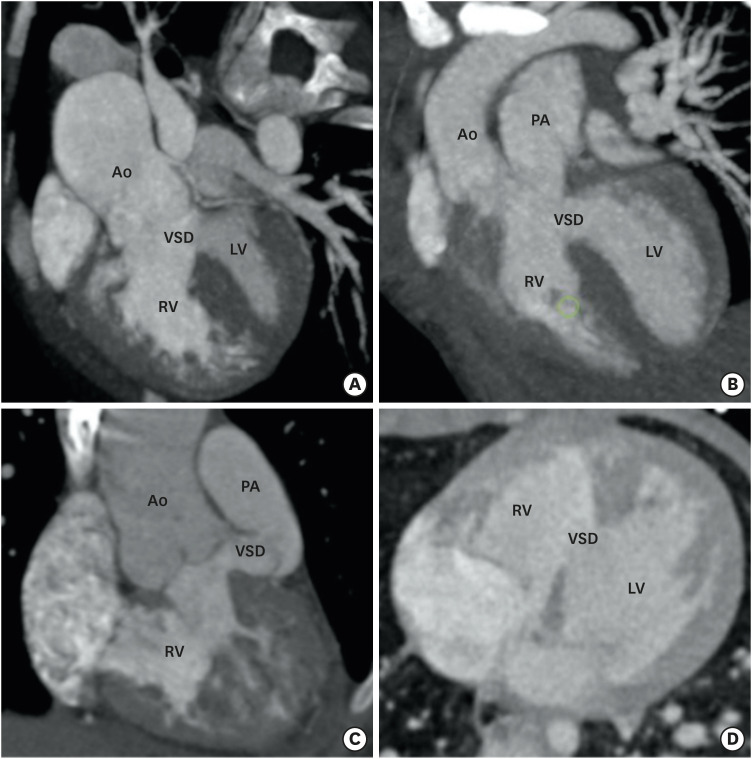
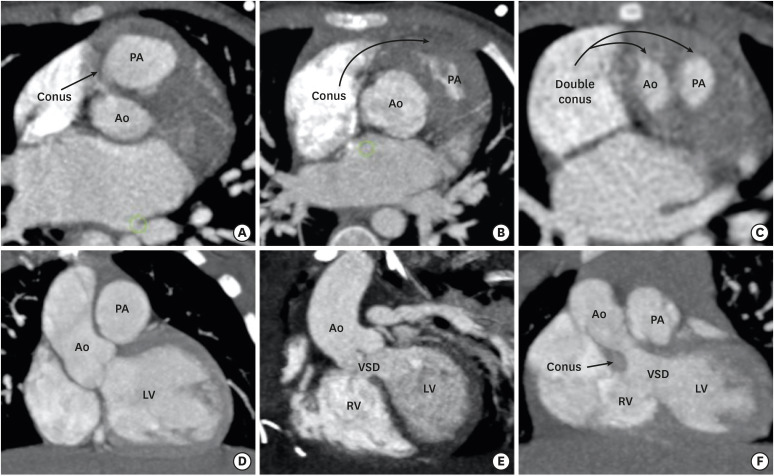
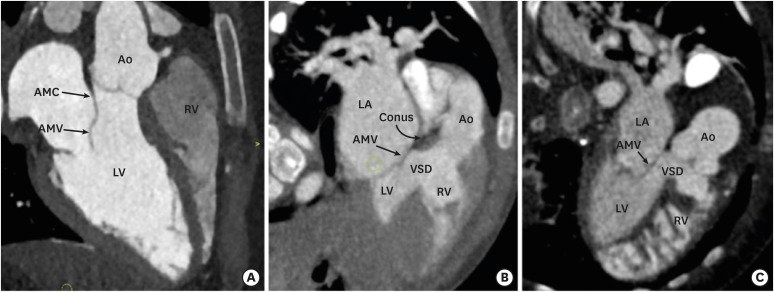
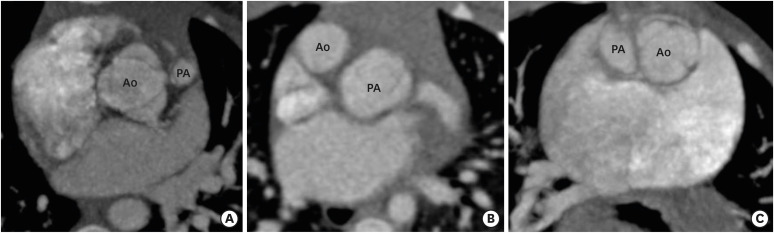
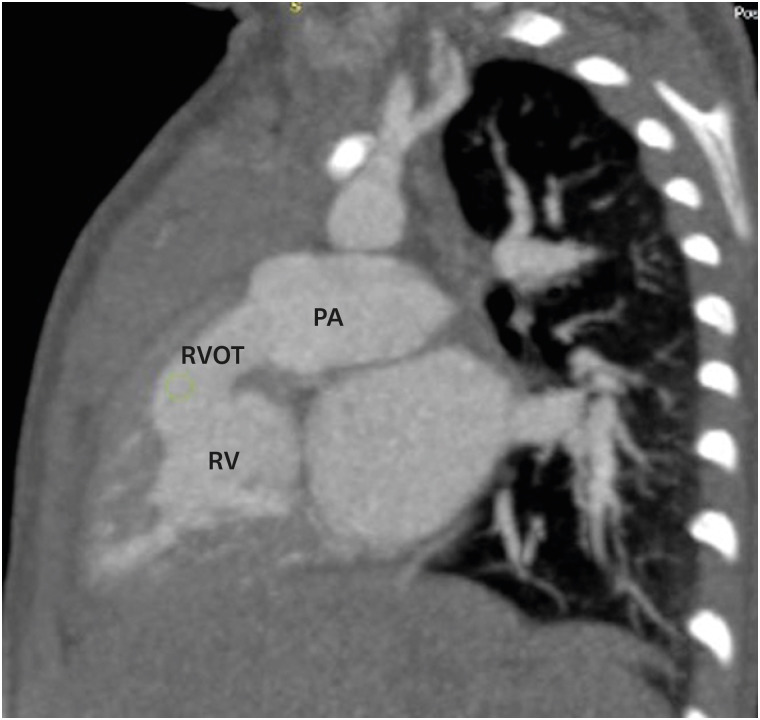
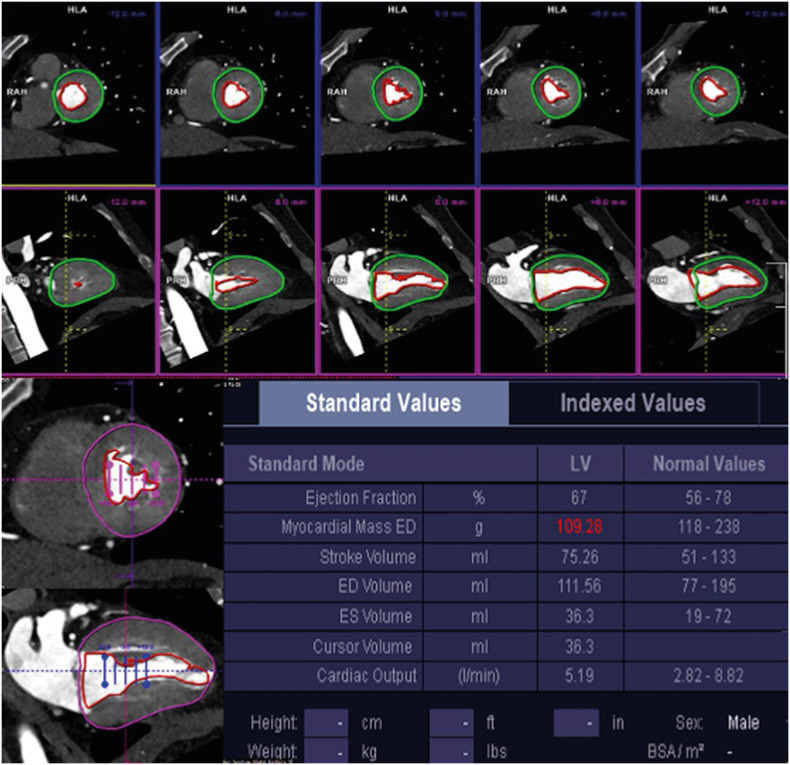
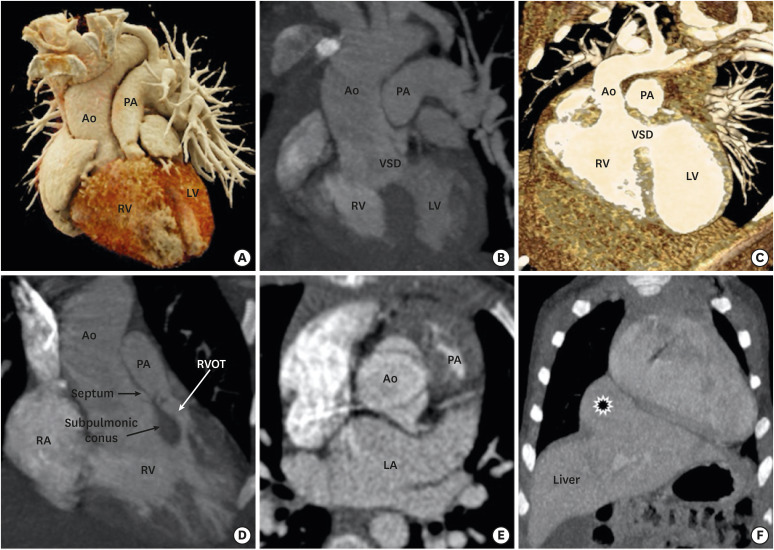
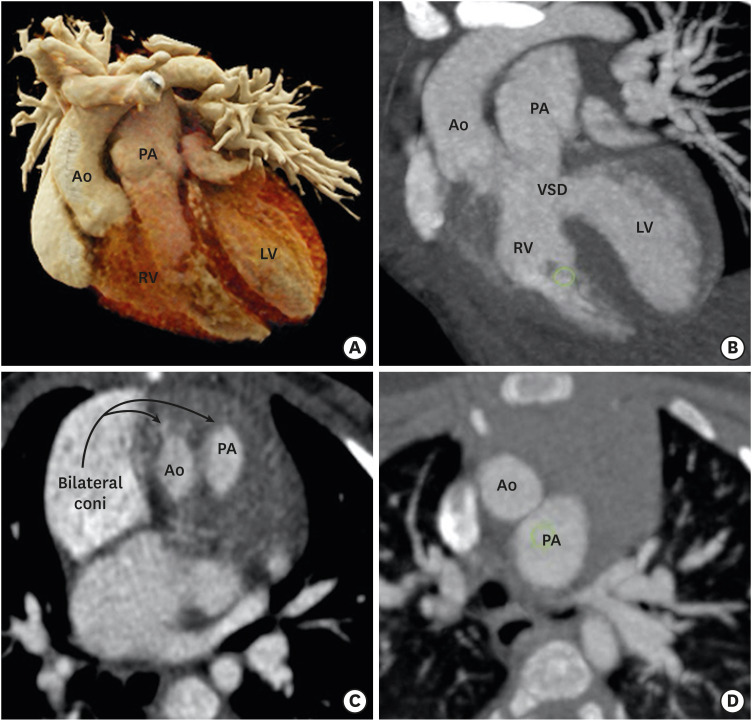
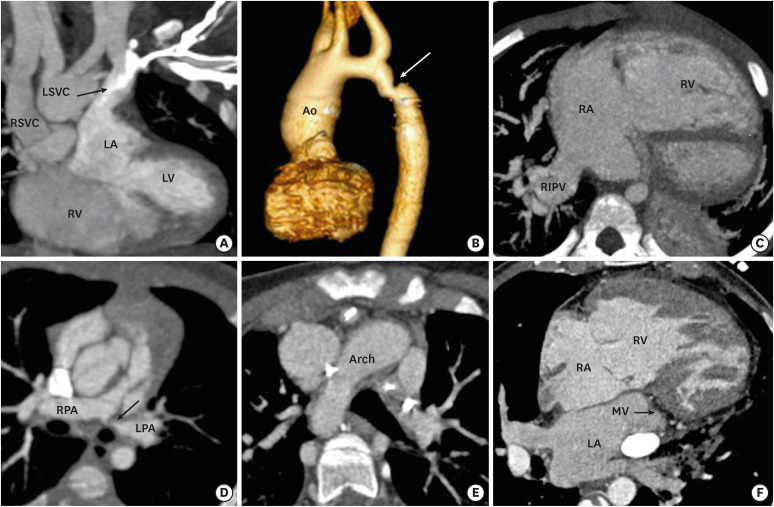
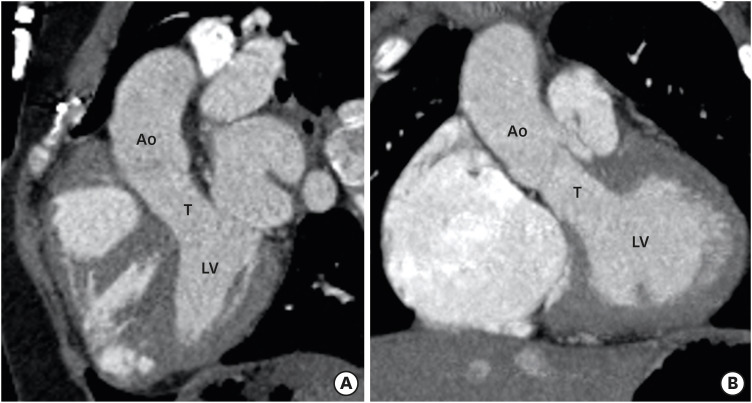
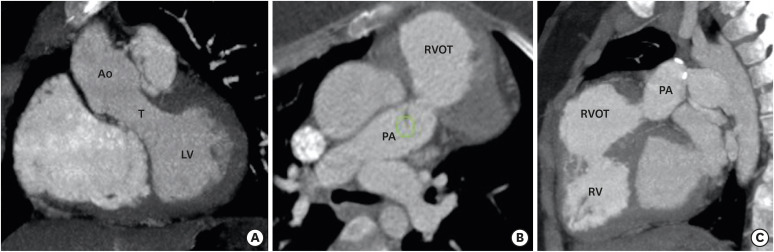
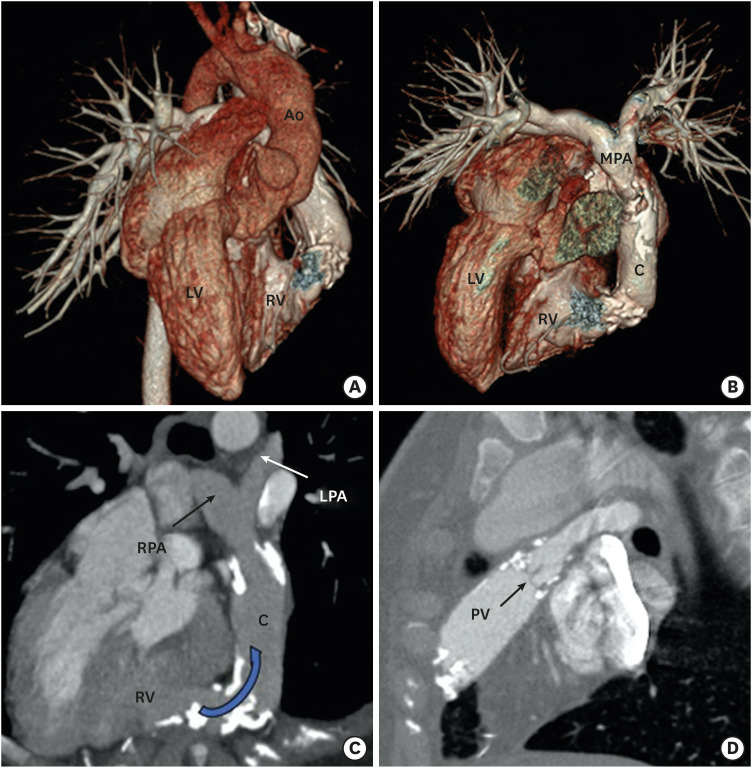
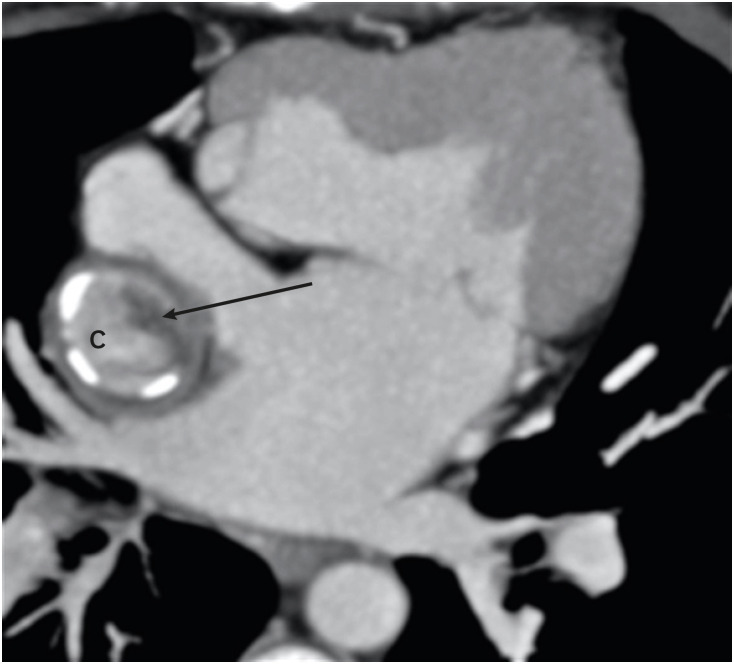
Double-outlet right ventricle (DORV) is a type of ventriculoarterial connection in which both great arteries arise entirely or predominantly from the right ventricle. The morphology of DORV is characterized by a ventricular septal defect (location and relationship with the semilunar valve); bilateral coni and aortomitral continuity; the presence or absence of outflow tract obstruction; tricuspid-pulmonary annular distance; and associated cardiac anomalies. The surgical approach varies with the type of DORV and is based on multiple variables. Computed tomography (CT) is a robust diagnostic tool for the preoperative and postoperative assessment of DORV. Unlike echocardiography and magnetic resonance imaging (MRI), CT imaging is not limited by small acoustic window, need for anaesthesia and can be used in patients with metallic implants. Current generations CT scanners with high spatial and temporal resolution, wide detectors, high-pitch scanning mode, dose-reduction algorithms, and advanced three-dimensional post-processing tools provide a low-risk, high-quality alternative to diagnostic cardiac catheterization or MRI, and have been increasingly utilized in nearly every type of congenital heart defect, including DORV.
Keywords: Congenital heart disease; Double outlet right ventricle.
Copyright © 2021 Korean Society of Echocardiography.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Walters HL, 3rd, Mavroudis C, Tchervenkov CI, Jacobs JP, Lacour-Gayet F, Jacobs ML. Congenital Heart Surgery Nomenclature and Database Project: double outlet right ventricle. Ann Thorac Surg. 2000;69:S249–63. - PubMed
-
- Smallhorn JF. Double-outlet right ventricle: an echocardiographic approach. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2000;3:20–33. - PubMed
-
- Elster A. Impact of new technologies on dose reduction in CT. In: Osborn AG, Abbara S, Elster AD, et al., editors. Yearbook of Diagnostic Radiology. St. Louis, MO: Mosby; 2011. pp. 191–192. - DOI
-
- Lacour-Gayet F, Haun C, Ntalakoura K, et al. Biventricular repair of double outlet right ventricle with non-committed ventricular septal defect (VSD) by VSD rerouting to the pulmonary artery and arterial switch. Eur J Cardiothorac Surg. 2002;21:1042–1048. - PubMed
-
- Sridaromont S, Feldt RH, Ritter DG, Davis GD, Edwards JE. Double outlet right ventricle: hemodynamic and anatomic correlations. Am J Cardiol. 1976;38:85–94. - PubMed
Publication types
LinkOut - more resources
Full Text Sources