Cardiac Decompression by Pericardiectomy for Constrictive Pericarditis: Multimodality Imaging to Identify Patients at Risk for Prolonged Inotropic Support
- PMID: 34080350
- PMCID: PMC8592688
- DOI: 10.4250/jcvi.2020.0223
Cardiac Decompression by Pericardiectomy for Constrictive Pericarditis: Multimodality Imaging to Identify Patients at Risk for Prolonged Inotropic Support
Abstract
Background: Post-pericardiectomy right ventricular (RV) failure has been reported but it remains not well-studied. To investigate imaging parameters that could predict RV function and the outcome of patients post-pericardiectomy.
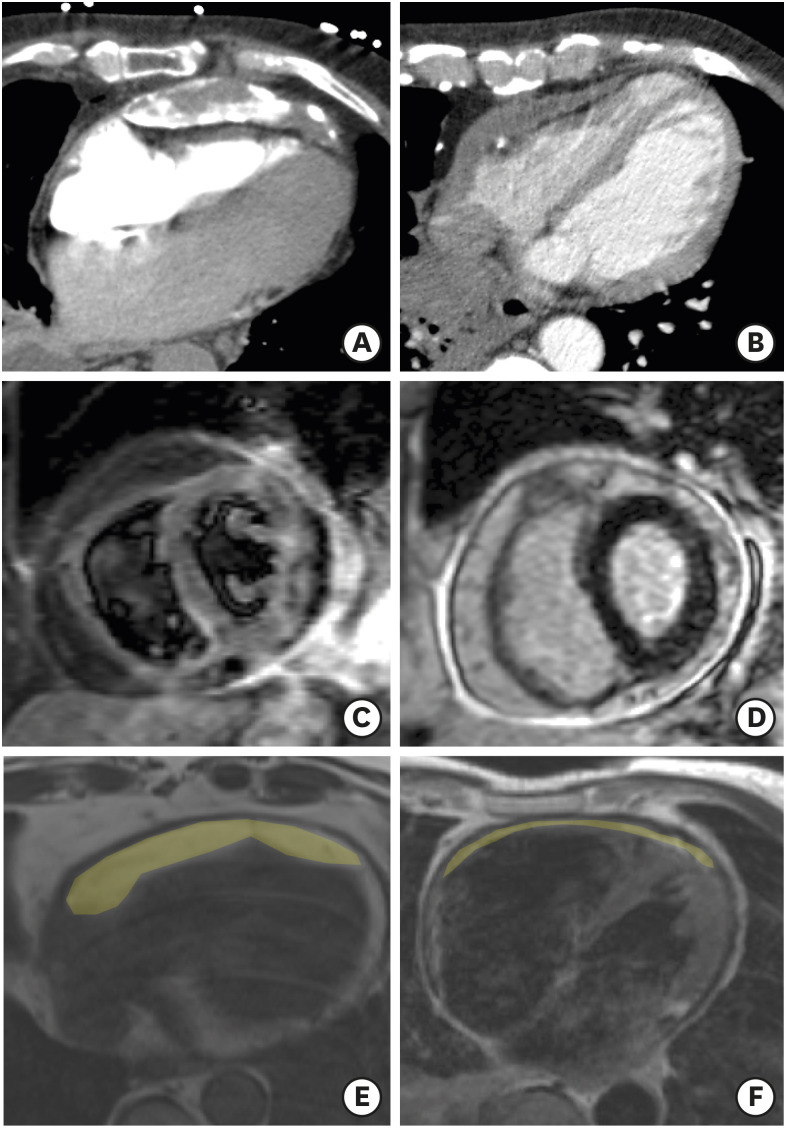
Methods: We analysed data from a total of 53 CP patients undergoing pericardiectomy. Preoperative, early and at 6 months postoperative echocardiographic (echo) imaging datasets were analysed and correlated with preoperative cardiac magnetic resonance (CMR), cardiac computed tomography scans and histology. The primary endpoint of the study was RV functional status early postoperatively and at 6 months. Secondary endpoint was the need for prolonged inotropic support.
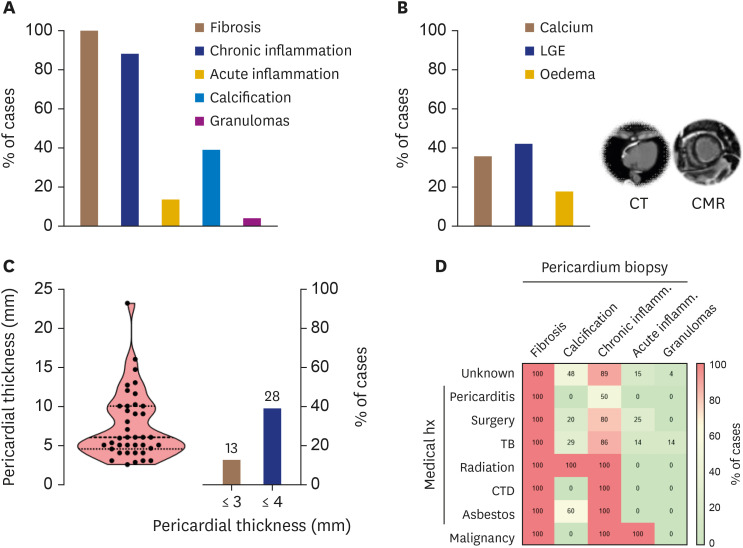
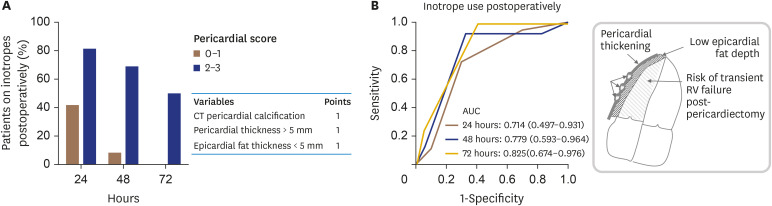
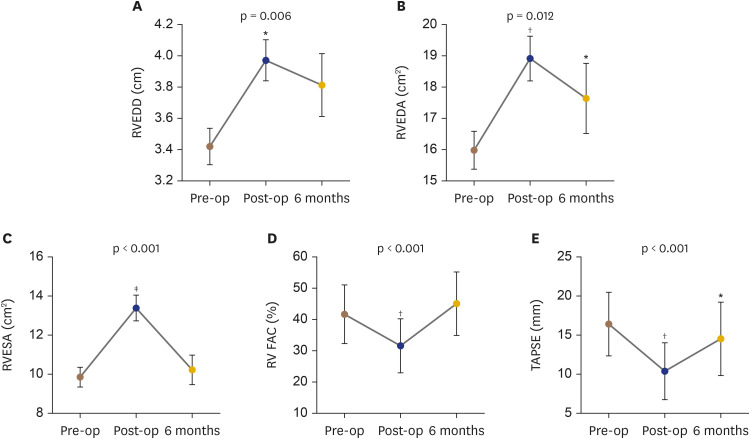
Results: A cause of CP was identified in 26 patients (49%). Inotropic support ≥ 48 hours was required in n = 28 (53%) of patients and was correlated with lower preoperative RV areas by echo or RV volumes by CMR (p < 0.05 for all). A pericardial score based on pericardial thickness/calcification and epicardial fat thickness had good diagnostic accuracy to identify patients requiring prolonged use of inotropes (area under the curve, 0.825; 95% confidence interval, 0.674-0.976). Pericardiectomy resulted in RV decompression and impaired RV function early postoperatively (fractional area change: 40.5% ± 8.8% preoperatively vs. 31.4% ± 10.4% early postoperatively vs. 42.5% ± 10.2% at 6 months, p < 0.001).
Conclusions: We show that a smaller RV cavity size and a pericardial scoring system are associated with prolonged inotropic support in CP patients undergoing pericardiectomy. RV systolic impairment post decompression is present in most patients, but it is only transient.
Keywords: Constrictive pericarditis; Echocardiography; Magnetic resonance; Multislice computed tomography; Pericardiectomy.
Copyright © 2021 Korean Society of Echocardiography.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Biventricular mechanics in constrictive pericarditis comparison with restrictive cardiomyopathy and impact of pericardiectomy.Circ Cardiovasc Imaging. 2013 May 1;6(3):399-406. doi: 10.1161/CIRCIMAGING.112.000078. Epub 2013 Mar 26. Circ Cardiovasc Imaging. 2013. PMID: 23532508
-
Transient right ventricular dysfunction after pericardiectomy in patients with constrictive pericarditis.Korean Circ J. 2011 May;41(5):283-6. doi: 10.4070/kcj.2011.41.5.283. Epub 2011 May 31. Korean Circ J. 2011. PMID: 21731572 Free PMC article.
-
Pericardial delayed hyperenhancement with CMR imaging in patients with constrictive pericarditis undergoing surgical pericardiectomy: a case series with histopathological correlation.JACC Cardiovasc Imaging. 2011 Nov;4(11):1180-91. doi: 10.1016/j.jcmg.2011.08.011. JACC Cardiovasc Imaging. 2011. PMID: 22093269
-
Surgical Treatment of Constrictive Pericarditis.Tex Heart Inst J. 2017 Apr 1;44(2):101-106. doi: 10.14503/THIJ-16-5772. eCollection 2017 Apr. Tex Heart Inst J. 2017. PMID: 28461794 Free PMC article. Review.
-
Constrictive Pericarditis: A Practical Clinical Approach.Prog Cardiovasc Dis. 2017 Jan-Feb;59(4):369-379. doi: 10.1016/j.pcad.2016.12.008. Epub 2017 Jan 4. Prog Cardiovasc Dis. 2017. PMID: 28062267 Review.
Cited by
-
Right ventricular dysfunction after pericardiectomy for tuberculous constrictive pericarditis: A case report.Clin Case Rep. 2024 May 23;12(6):e8899. doi: 10.1002/ccr3.8899. eCollection 2024 Jun. Clin Case Rep. 2024. PMID: 38799540 Free PMC article.
-
Post-pericardiectomy ECMO for constrictive pericarditis: a case series and literature review.BMC Anesthesiol. 2025 Mar 1;25(1):110. doi: 10.1186/s12871-025-02977-4. BMC Anesthesiol. 2025. PMID: 40025418 Free PMC article. Review.
-
Novel Imaging Parameters for Right Ventricular Dysfunction after Pericardiectomy in Constrictive Pericarditis.J Cardiovasc Imaging. 2021 Oct;29(4):373-374. doi: 10.4250/jcvi.2021.0074. Epub 2021 May 24. J Cardiovasc Imaging. 2021. PMID: 34080353 Free PMC article. No abstract available.
-
Multimodality Imaging of Constrictive Pericarditis: Pathophysiology and New Concepts.Curr Cardiol Rep. 2022 Oct;24(10):1439-1453. doi: 10.1007/s11886-022-01758-6. Epub 2022 Aug 2. Curr Cardiol Rep. 2022. PMID: 35917048 Free PMC article. Review.
References
-
- Frank H, Globits S. Magnetic resonance imaging evaluation of myocardial and pericardial disease. J Magn Reson Imaging. 1999;10:617–626. - PubMed
-
- Young PM, Glockner JF, Williamson EE, et al. MR imaging findings in 76 consecutive surgically proven cases of pericardial disease with CT and pathologic correlation. Int J Cardiovasc Imaging. 2012;28:1099–1109. - PubMed
-
- Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation. 1999;100:1380–1386. - PubMed
-
- Beckmann E, Ismail I, Cebotari S, et al. Right-sided heart failure and extracorporeal life support in patients undergoing pericardiectomy for constrictive pericarditis: a risk factor analysis for adverse outcome. Thorac Cardiovasc Surg. 2017;65:662–670. - PubMed