

Comparative Genomic Analysis of Intrahepatic Cholangiocarcinoma: Biopsy Type, Ancestry, and Testing Patterns
- PMID: 34080753
- PMCID: PMC8417854
- DOI: 10.1002/onco.13844
Comparative Genomic Analysis of Intrahepatic Cholangiocarcinoma: Biopsy Type, Ancestry, and Testing Patterns
Abstract
Background: At diagnosis, the majority of patients with intrahepatic cholangiocarcinoma (IHCC) present with advanced disease and a poor prognosis. Comprehensive genomic profiling (CGP) early in the disease course may increase access to targeted therapies and clinical trials; however, unresolved issues remain surrounding the optimal biopsy type to submit for CGP.
Patients and methods: Mutational frequencies between primary tumor biopsies (Pbx), metastatic biopsies (Mbx), and liquid biopsies (Lbx) in 1,632 patients with IHCC were compared.
Results: Potentially actionable alterations were found in 52%, 34%, and 35% of patients in the Pbx, Mbx, and Lbx cohorts, respectively. In Pbx, Mbx, and Lbx, FGFR2 rearrangements were found in 9%, 6%, and 4%, and IDH1 mutations were identified in 16%, 5%, and 9% patients, respectively. Moreover, alterations in FGFR2 and IDH1 were significantly associated with distinct ancestries, including 2.1-fold enrichment for FGFR2 rearrangements in patients with African ancestry and 1.5-fold enrichment for IDH1 mutations in patients with admixed American (Hispanic) ancestry. Finally, the publication of biomarker-driven clinical trials in IHCC correlated with changing CGP testing patterns. Significant correlations between patient characteristics and IHCC trial disclosures were observed, including a significant decrease from time between biopsy and CGP testing, and more frequent testing of primary versus metastatic samples.
Conclusion: Overall, because of the high likelihood of identifying actionable genomic alterations, CGP should be considered for the majority of patients with inoperable IHCC, and Lbx and Mbx can be considered as part of the diagnostic suite.
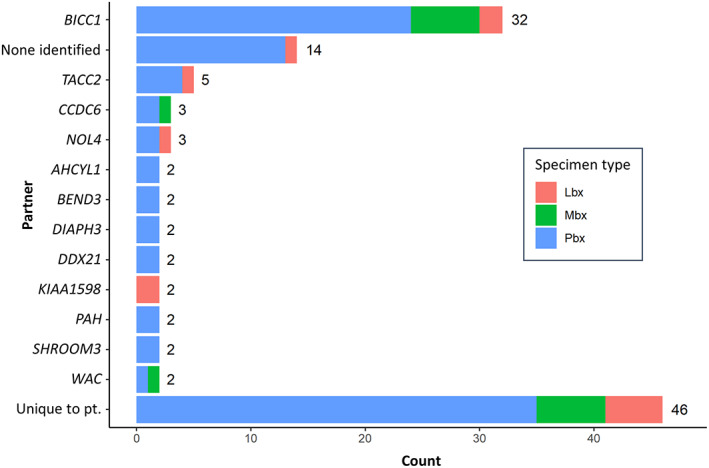
Implications for practice: Comprehensive genomic profiling (CGP) should be considered for all patients with intrahepatic cholangiocarcinoma (IHCC) or suspected IHCC, as actionable alterations were commonly found in multiple genes and a wide variety of FGFR2 fusion partners were identified. The disclosure of IHCC trial data correlated with increased use of CGP, an encouraging trend that moves new therapeutic options forward for rare cancers with a rare biomarker. Although tissue from the primary lesion may identify actionable alterations at higher rates, CGP of a liquid biopsy or metastatic site can be considered, particularly if the primary tissue block is exhausted.
Keywords: Bile duct neoplasms; Comparative genomics; Intrahepatic cholangiocarcinoma; Liquid biopsy.
© 2021 AlphaMed Press.
Conflict of interest statement
Figures



References
-
- Mukkamalla SKR, Naseri HM, Kim BM et al. Trends in incidence and factors affecting survival of patients with cholangiocarcinoma in the United States. J Natl Compr Canc Netw 2018;16:370–376. - PubMed
-
- Bridgewater J, Galle PR, Khan SA et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol 2014;60:1268–1289. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
