

Mirtazapine reduces susceptibility to hypocapnic central sleep apnea in males with sleep-disordered breathing: a pilot study
- PMID: 34080920
- PMCID: PMC8325612
- DOI: 10.1152/japplphysiol.00838.2020
Mirtazapine reduces susceptibility to hypocapnic central sleep apnea in males with sleep-disordered breathing: a pilot study
Abstract
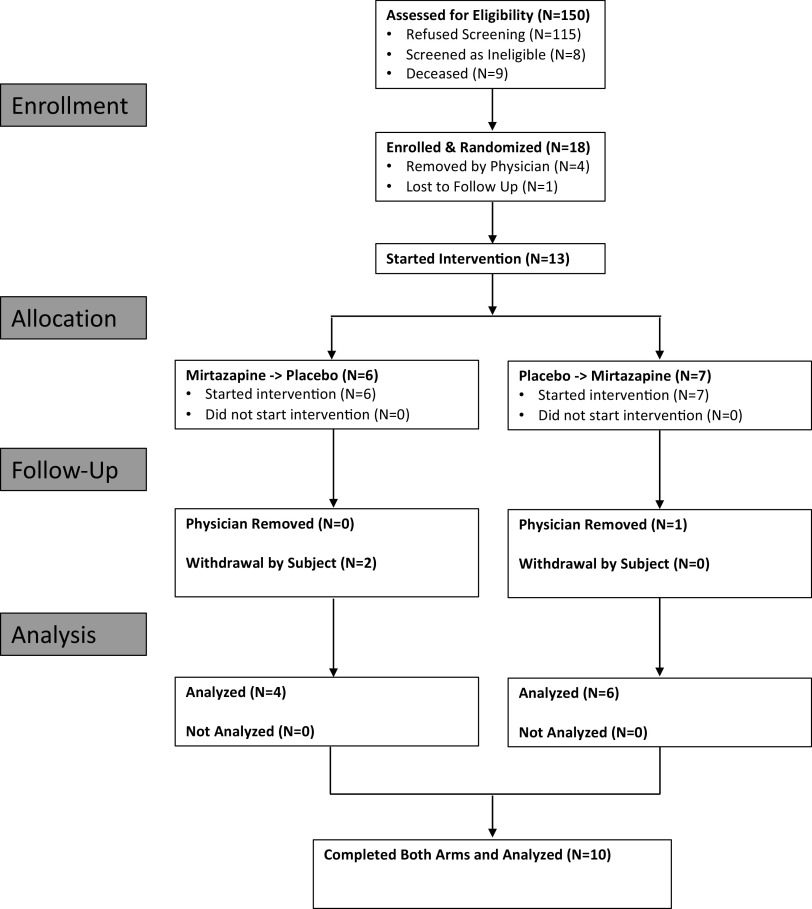
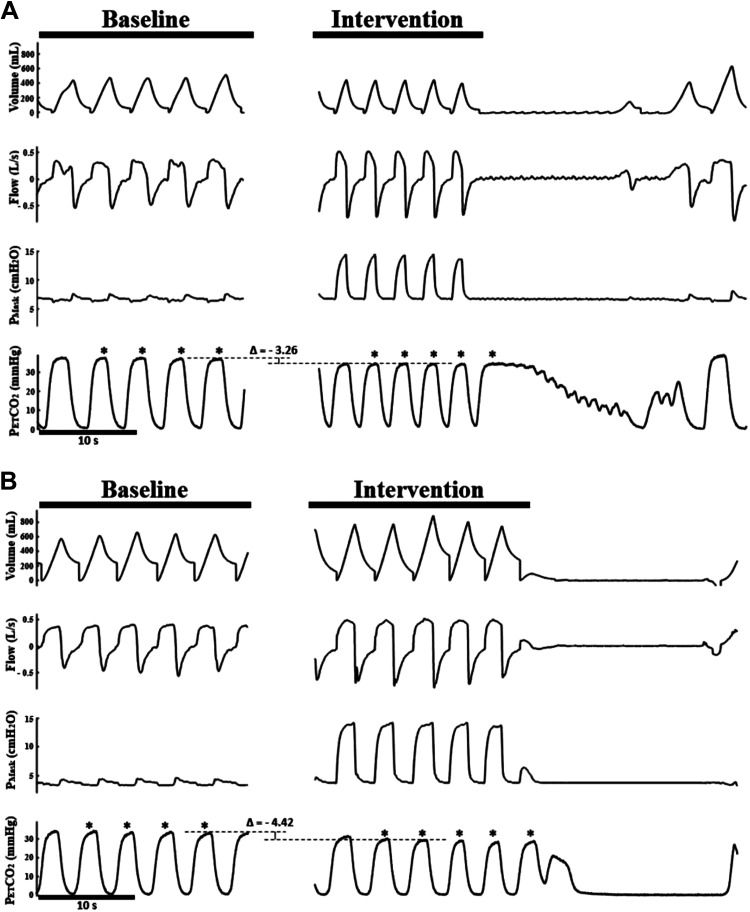
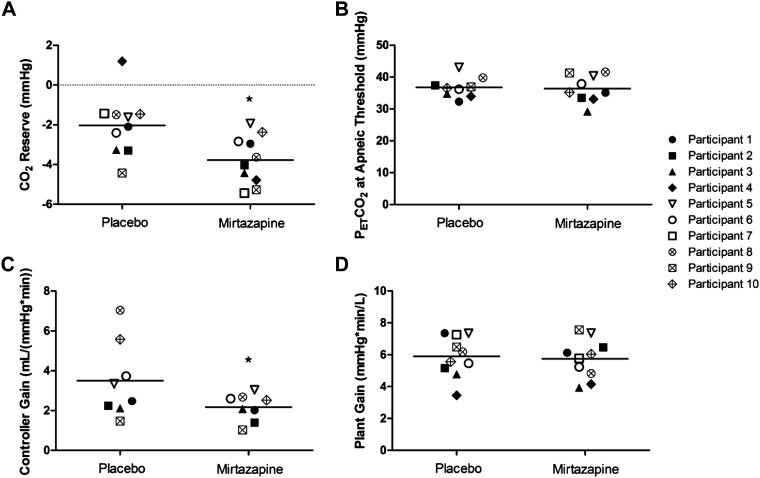
Studies in humans and animal models with spinal cord injury (SCI) have demonstrated that medications targeting serotonin receptors may decrease the susceptibility to central sleep-disordered breathing (SDB). We hypothesized that mirtazapine would decrease the propensity to develop hypocapnic central sleep apnea (CSA) during sleep. We performed a single-blind pilot study on a total of 10 men with SDB (7 with chronic SCI and 3 noninjured) aged 52.0 ± 11.2 yr. Participants were randomly assigned to either mirtazapine (15 mg at bedtime) or a placebo for at least 1 wk, followed by a 7-day washout period before crossing over to the other intervention. Split-night studies included polysomnography and induction of hypocapnic CSA using a noninvasive ventilation (NIV) protocol. The primary outcome was CO2 reserve, defined as the difference between eupneic and end of NIV end-tidal CO2 ([Formula: see text]) preceding induced hypocapneic CSA. Secondary outcomes included controller gain (CG), other ventilatory parameters, and SDB severity. CG was defined as the ratio of change in minute ventilation (V̇e) between control and hypopnea to the change in CO2 during sleep. CO2 reserve was significantly widened on mirtazapine than placebo (-3.8 ± 1.2 vs. -2.0 ± 1.5 mmHg; P = 0.015). CG was significantly decreased on mirtazapine compared with placebo [2.2 ± 0.7 vs. 3.5 ± 1.9 L/(mmHg × min); P = 0.023]. There were no significant differences for other ventilatory parameters assessed or SDB severity between mirtazapine and placebo trials. These findings suggest that the administration of mirtazapine can decrease the susceptibility to central apnea by reducing chemosensitivity and increasing CO2 reserve; however, considering the lack of changes in apnea-hypopnea index (AHI), further research is required to understand the significance of this finding.NEW & NOTEWORTHY To our knowledge, this research study is novel as it is the first study in humans assessing the effect of mirtazapine on CO2 reserve and chemosensitivity in individuals with severe sleep-disordered breathing. This is also the first study to determine the potential therapeutic effects of mirtazapine on sleep parameters in individuals with a spinal cord injury.
Keywords: CO2 reserve; central sleep apnea; mirtazapine; sleep disordered-breathing; spinal cord injury.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Kushida CA, Littner MR, Hirshkowitz M, Morgenthaler TI, Alessi CA, Bailey D, Boehlecke B, Brown TM, Coleman J, Friedman L, Kapen S, Kapur VK, Kramer M, Lee-Chiong T, Owens J, Pancer JP, Swick TJ, Wise MS; American Academy of Sleep Medicine. Practice param4 eters for the use of continuous and bilevel positive airway pressure de4 vices to treat adult patients with sleep4related breathing disorders. Sleep 29: 375–380, 2006. doi: 10.1093/sleep/29.3.375. - DOI - PubMed
-
- Aurora RN, Chowdhuri S, Ramar K, Bista SR, Casey KR, Lamm CI, Kristo DA, Mallea JM, Rowley JA, Zak RS, Tracy SL. The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses. Sleep 35: 17–40, 2012. doi: 10.5665/sleep.1580. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical