

A Fully Integrated Closed-Loop System Based on Mesoporous Microneedles-Iontophoresis for Diabetes Treatment
- PMID: 34081407
- PMCID: PMC8373098
- DOI: 10.1002/advs.202100827
A Fully Integrated Closed-Loop System Based on Mesoporous Microneedles-Iontophoresis for Diabetes Treatment
Abstract
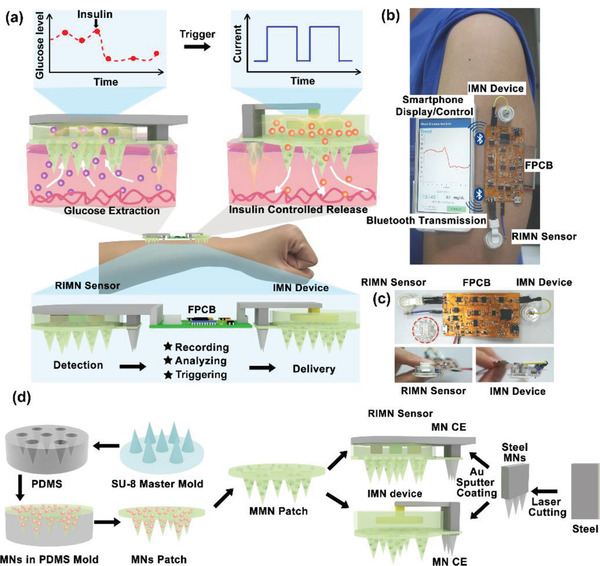
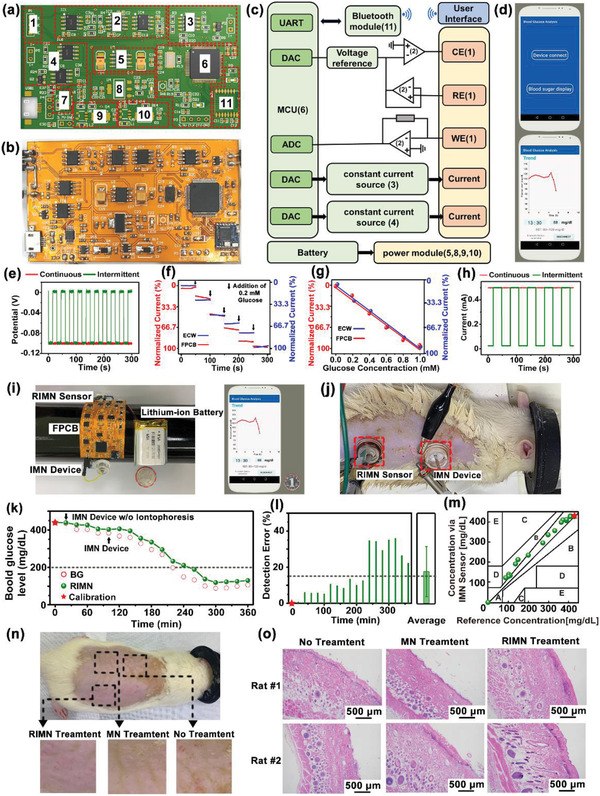
A closed-loop system that can mini-invasively track blood glucose and intelligently treat diabetes is in great demand for modern medicine, yet it remains challenging to realize. Microneedles technologies have recently emerged as powerful tools for transdermal applications with inherent painlessness and biosafety. In this work, for the first time to the authors' knowledge, a fully integrated wearable closed-loop system (IWCS) based on mini-invasive microneedle platform is developed for in situ diabetic sensing and treatment. The IWCS consists of three connected modules: 1) a mesoporous microneedle-reverse iontophoretic glucose sensor; 2) a flexible printed circuit board as integrated and control; and 3) a microneedle-iontophoretic insulin delivery component. As the key component, mesoporous microneedles enable the painless penetration of stratum corneum, implementing subcutaneous substance exchange. The coupling with iontophoresis significantly enhances glucose extraction and insulin delivery and enables electrical control. This IWCS is demonstrated to accurately monitor glucose fluctuations, and responsively deliver insulin to regulate hyperglycemia in diabetic rat model. The painless microneedles and wearable design endows this IWCS as a highly promising platform to improve the therapies of diabetic patients.
Keywords: closed-loop system; diabetes monitor and therapy; intelligent wearable device; mesoporous microneedles-iontophoresis; minimally invasive.
© 2021 The Authors. Advanced Science published by Wiley-VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- a) Reddy B., Hassan U., Seymour C., Angus D. C., Isbell T. S., White K., Weir W., Yeh L., Vincent A., Bashir R., Nat. Biomed. Eng. 2018, 2, 640; - PubMed
- b) Min J., Chin L. K., Oh J., Landeros C., Vinegoni C., Lee J., Lee S. J., Park J. Y., Liu A.‐Q., Castro C. M., Lee H., Im H., Weissleder R., Sci. Transl. Med. 2020, 12, eaaz9746; - PMC - PubMed
- c) Laksanasopin T., Guo T. W., Nayak S., Sridhara A. A., Xie S., Olowookere O. O., Cadinu P., Meng F., Chee N. H., Kim J., Chin C. D., Munyazesa E., Mugwaneza P., Rai A. J., Mugisha V., Castro A. R., Steinmiller D., Linder V., Justman J. E., Nsanzimana S., Sia S. K., Sci. Transl. Med. 2015, 7, 273re1; - PubMed
- d) del Río J. S., Henry O. Y. F., Jolly P., Ingber D. E., Nat. Nanotechnol. 2019, 14, 1143. - PubMed
-
- a) Veiseh O., Tang B. C., Whitehead K. A., Anderson D. G., Langer R., Nat. Rev. Drug Discovery 2015, 14, 45; - PMC - PubMed
- b) Yu J., Wang J., Zhang Y., Chen G., Mao W., Ye Y., Kahkoska A. R., Buse J. B., Langer R., Gu Z., Nat. Biomed. Eng. 2020, 4, 499; - PMC - PubMed
- c) Bhatt D. L., Szarek M., Pitt B., Cannon C. P., Leiter L. A., McGuire D. K., Lewis J. B., Riddle M. C., Inzucchi S. E., Kosiborod M. N., Cherney D. Z. I., Dwyer J. P., Scirica B. M., Bailey C. J., Díaz R., Ray K. K., Udell J. A., Lopes R. D., Lapuerta P., Steg P. G., N. Engl. J. Med. 2020, 384, 129;
- d) Wang Y., Wang C., Li K., Song X., Yan X., Yu L., He Z., J. Controlled Release 2021, 330, 618. - PubMed
-
- a) Aye T., Block J., Buckingham B., Endocrinol. Metab. Clin. North Am. 2010, 39, 609; - PMC - PubMed
- b) Hovorka R., Leelarathna L., Eur. Endocrinol. 2010, 6, 58.
- c) Brown S. A., Kovatchev B. P., Raghinaru D., Lum J. W., Buckingham B. A., Kudva Y. C., Laffel L. M., Levy C. J., Pinsker J. E., Wadwa R. P., Dassau E., F. J.Doyle, 3rd, Anderson S. M., Church M. M., Dadlani V., Ekhlaspour L., Forlenza G. P., Isganaitis E., Lam D. W., Kollman C., Beck R. W., N. Engl. J. Med. 2019, 381, 1707; - PMC - PubMed
- d) Elleri D., Dunger D. B., Hovorka R., BMC Med. 2011, 9, 120. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 61771498/National Natural Science Foundation of China
- 82061148011/National Natural Science Foundation of China
- 81970778/National Natural Science Foundation of China
- 61901535/National Natural Science Foundation of China
- 31900954/National Natural Science Foundation of China
- 2020A1515010665/Guangdong Basic and Applied Basic Research Foundation
- 2020A1515010987/Guangdong Basic and Applied Basic Research Foundation
- 76120-18841213/100 Talents Program of Sun Yat-sen University
- 20lgpy47/Basic Scientific Research Special Foundation of Sun Yat-sen University
- 2020B1212060033/Funds of department of Science and Technology of Guangdong province and the Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science
- 2020M683079/China Postdoctoral Science Foundation
- SKT2006/Chinese Academy of Sciences Opening Project
LinkOut - more resources
Full Text Sources
Medical
Research Materials