

Revision Surgery and Progression to Total Hip Arthroplasty After Surgical Correction of Femoroacetabular Impingement: A Systematic Review
- PMID: 34081552
- PMCID: PMC8980457
- DOI: 10.1177/03635465211011744
Revision Surgery and Progression to Total Hip Arthroplasty After Surgical Correction of Femoroacetabular Impingement: A Systematic Review
Abstract
Background: Femoroacetabular impingement (FAI) is a major cause of hip pain in young adults and athletes. Surgical treatment of FAI is recommended in cases of failed nonoperative treatment that have the typical clinical and radiographic findings. At present, the role of risk factors for revision surgery and progression to total hip arthroplasty (THA) in patients with FAI is still unclear.
Purpose: To investigate the possible association between (1) rate of revision and progression to THA and (2) patient characteristics, type of lesion, family history of hip disease, type of intervention, radiographic parameters, physical examination, and pre- and postoperative scores.
Study design: Systematic review; Level of evidence, 4.
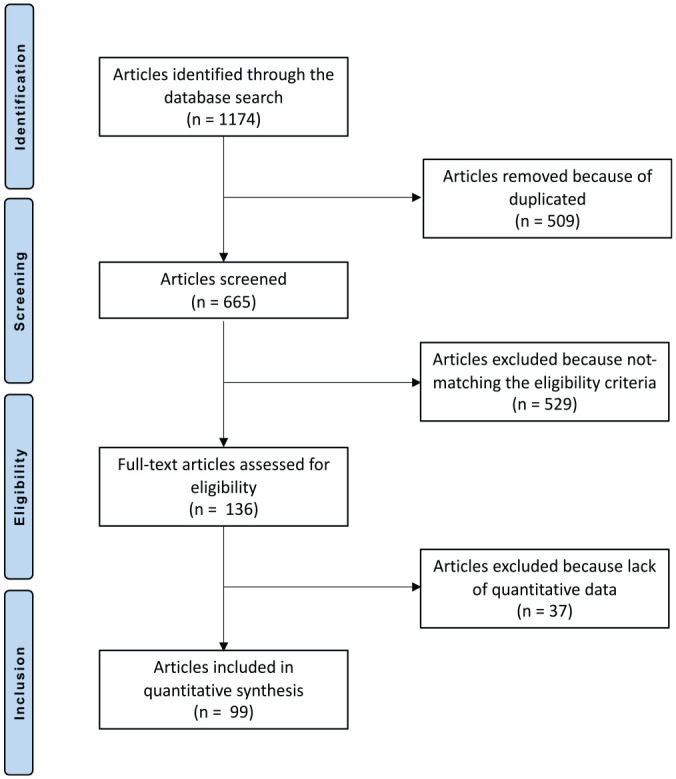
Methods: The present systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. In October 2020, the main online databases were accessed. All articles concerning surgical correction for selected patients with FAI were accessed. Patient characteristics, type of intervention, radiographic parameters, physical examination, and pre- and postoperative scores were assessed. The outcomes of interest were the possible association between these variables and the rate of revision and subsequent progression to THA using a multivariate analysis through the Pearson product-moment correlation coefficient.
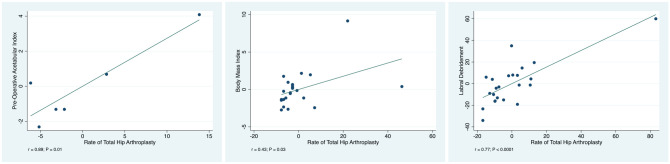
Results: Data from 99 studies (9357 procedures) were collected. The median follow-up was 30.9 months (interquartile range, 24.0-45.0). The mean ± SD age was 33.4 ± 9.3 years; mean body mass index (BMI), 24.8 ± 4.8; percentage right side, 55.8% ± 8.0%; and percentage female sex, 47.5% ± 20.4%. The overall rate of revision was 5.29% (351 of 6641 patients), while the rate of subsequent progression to THA was 3.78% (263 of 6966 patients). Labral debridement (P < .0001), preoperative acetabular index (P = .01), and BMI (P = .03) all showed evidence of a statistically positive association with increased rates of THA. No other statistically significant associations were found between patient characteristics, type of lesion, family history of hip disease, type of intervention, radiographic parameters, physical examination, or pre- and postoperative scores and the rate of revision and/or progression to THA.
Conclusion: Although surgical procedures to treat FAI led to satisfactory outcomes, there was a revision rate of 5.29% in the 9357 procedures in the present systematic review. The rate of progression to THA after a median follow-up of 30 months was 3.78%. Patients who have a higher BMI and/or have a pathologic acetabular index and/or undergo labral debridement during correction of FAI are more at risk for a subsequent THA. We advocate additional education of this patient population in terms of expected outcomes and suggest surgical labral repair instead of debridement if needed.
Keywords: femoroacetabular impingement; revision surgery; risk factors; total hip arthroplasty.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
What Are the Risk Factors for Revision Surgery After Hip Arthroscopy for Femoroacetabular Impingement at 7-year Followup?Clin Orthop Relat Res. 2017 Apr;475(4):1169-1177. doi: 10.1007/s11999-016-5115-6. Clin Orthop Relat Res. 2017. PMID: 27718121 Free PMC article.
-
High Risk of Conversion to THA After Femoroacetabular Osteoplasty for Femoroacetabular Impingement in Patients Older than 40 Years.Clin Orthop Relat Res. 2021 May 1;479(5):1112-1118. doi: 10.1097/CORR.0000000000001554. Clin Orthop Relat Res. 2021. PMID: 33236866 Free PMC article.
-
Association Between Chondrolabral Junction Breakdown and Conversion to Total Hip Arthroplasty After Hip Arthroscopy for Symptomatic Labral Tears: Minimum 8-Year Follow-up.Am J Sports Med. 2024 Apr;52(5):1153-1164. doi: 10.1177/03635465241234258. Epub 2024 Mar 12. Am J Sports Med. 2024. PMID: 38476016 Free PMC article.
-
Surgical Outcomes in the Treatment of Concomitant Mild Acetabular Dysplasia and Femoroacetabular Impingement: A Systematic Review.Arthroscopy. 2020 Apr;36(4):1176-1184. doi: 10.1016/j.arthro.2019.11.122. Epub 2019 Dec 4. Arthroscopy. 2020. PMID: 31809799
-
Outcomes of arthroscopy of the hip for femoroacetabular impingement based on intraoperative assessment using the Outerbridge classification.Bone Joint J. 2023 Jul 1;105-B(7):751-759. doi: 10.1302/0301-620X.105B7.BJJ-2022-0989.R1. Bone Joint J. 2023. PMID: 37399116
Cited by
-
Hyperlipidemia does not influence clinical outcome in arthroscopic treatment of femoroacetabular impingement syndrome.J Orthop Surg Res. 2022 Aug 31;17(1):398. doi: 10.1186/s13018-022-03290-3. J Orthop Surg Res. 2022. PMID: 36045389 Free PMC article.
-
Risk factors for liner wear and head migration in total hip arthroplasty: a systematic review.Sci Rep. 2023 Sep 20;13(1):15612. doi: 10.1038/s41598-023-42809-4. Sci Rep. 2023. PMID: 37730762 Free PMC article.
-
Current understanding of articular cartilage lesions in femoroacetabular impingement syndrome.J Orthop Surg Res. 2024 Dec 30;19(1):886. doi: 10.1186/s13018-024-05322-6. J Orthop Surg Res. 2024. PMID: 39734214 Free PMC article. Review.
-
Patient Factors Influencing Outcomes at 12-Year Follow-up of Hip Arthroscopy for Femoroacetabular Impingement.Am J Sports Med. 2024 Aug;52(10):2586-2595. doi: 10.1177/03635465241265721. Epub 2024 Aug 13. Am J Sports Med. 2024. PMID: 39137412 Free PMC article.
-
Conservative therapy versus arthroscopic surgery of femoroacetabular impingement syndrome (FAI): a systematic review and meta-analysis.J Orthop Surg Res. 2022 Jun 3;17(1):296. doi: 10.1186/s13018-022-03187-1. J Orthop Surg Res. 2022. PMID: 35659016 Free PMC article.
References
-
- Bardakos NV, Vasconcelos JC, Villar RN. Early outcome of hip arthroscopy for femoroacetabular impingement: the role of femoral osteoplasty in symptomatic improvement. J Bone Joint Surg Br. 2008;90(12):1570-1575. - PubMed
-
- Beaulé PE, Le Duff MJ, Zaragoza E. Quality of life following femoral head-neck osteochondroplasty for femoroacetabular impingement. J Bone Joint Surg Am. 2007;89(4):773-779. - PubMed
-
- Beck M, Buchler L. Prevalence and impact of pain at the greater trochanter after open surgery for the treatment of femoro-acetabular impingement. J Bone Joint Surg Am. 2011;93(suppl 2):66-69. - PubMed
-
- Beck M, Leunig M, Parvizi J, et al.. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004;418:67-73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
