

Epitope-specific antibody responses differentiate COVID-19 outcomes and variants of concern
- PMID: 34081630
- PMCID: PMC8410046
- DOI: 10.1172/jci.insight.148855
Epitope-specific antibody responses differentiate COVID-19 outcomes and variants of concern
Abstract
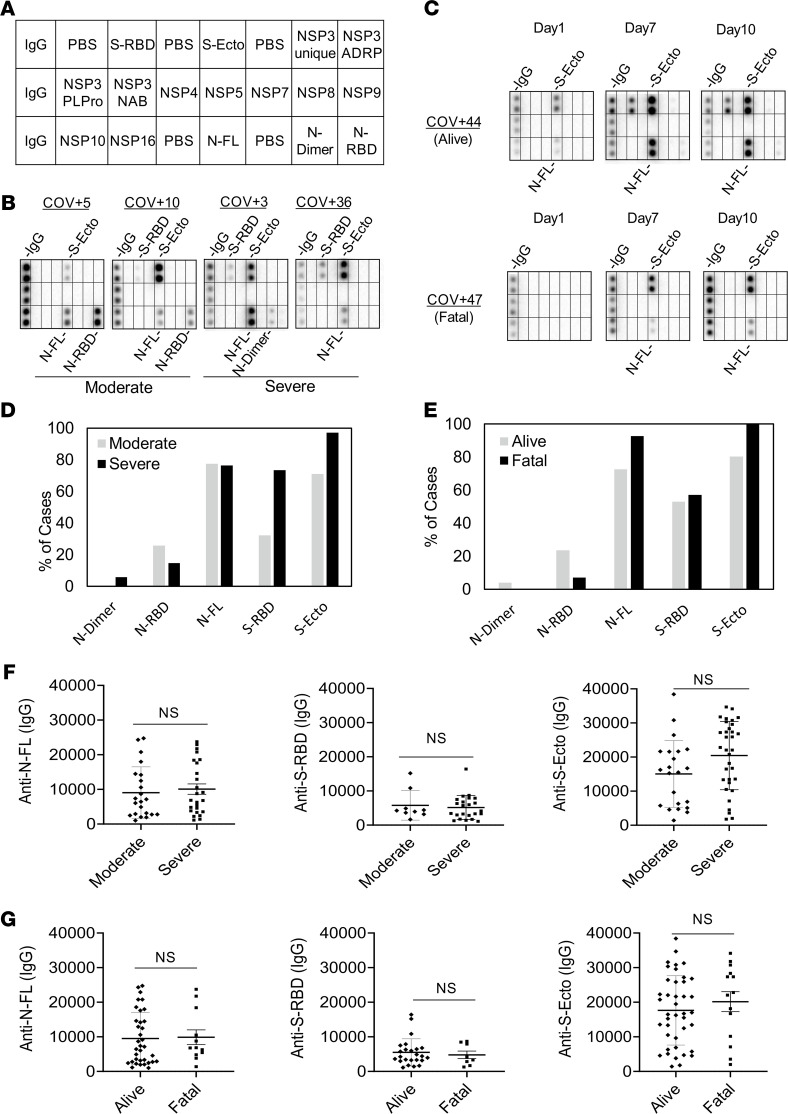
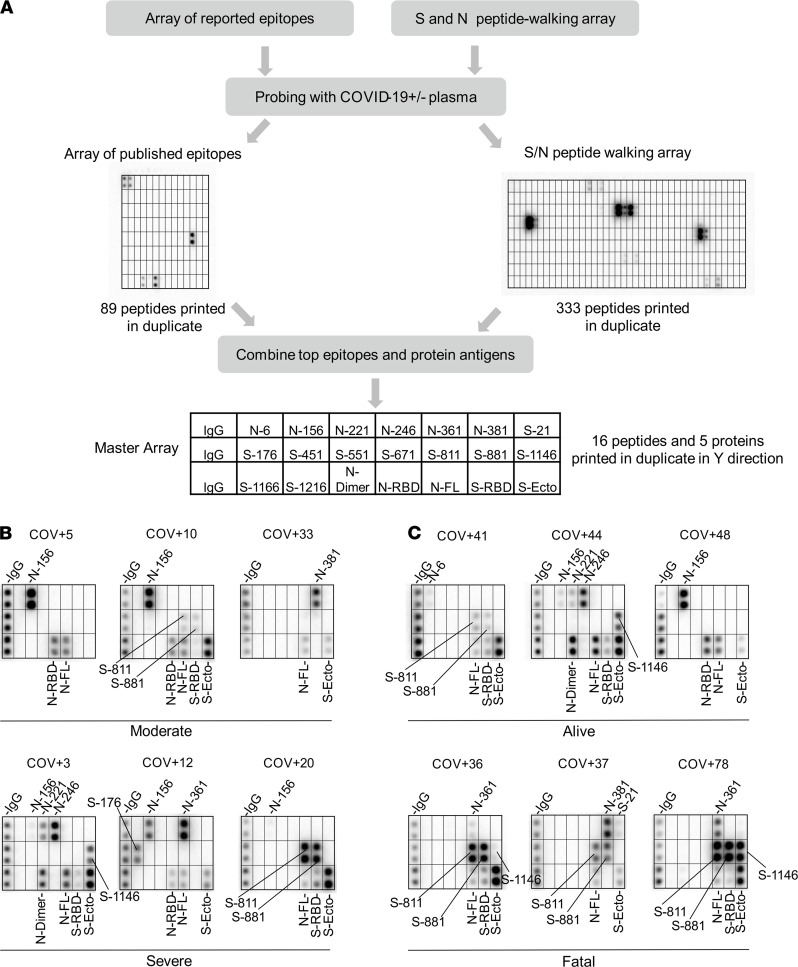
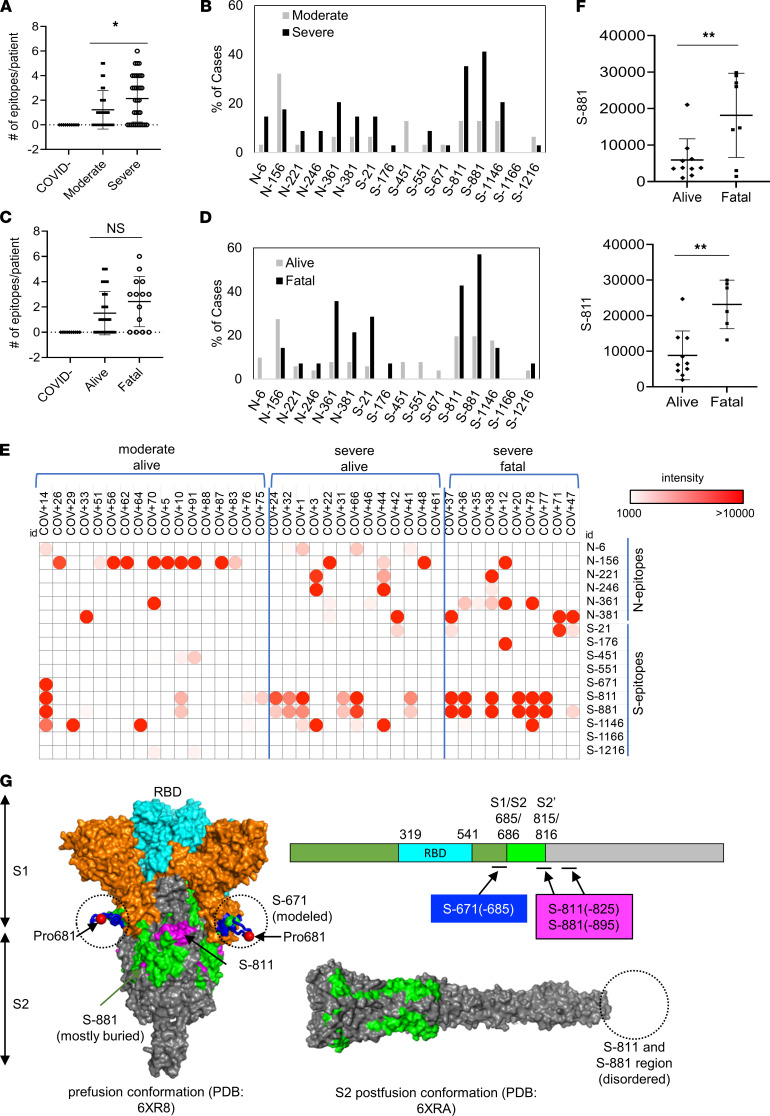
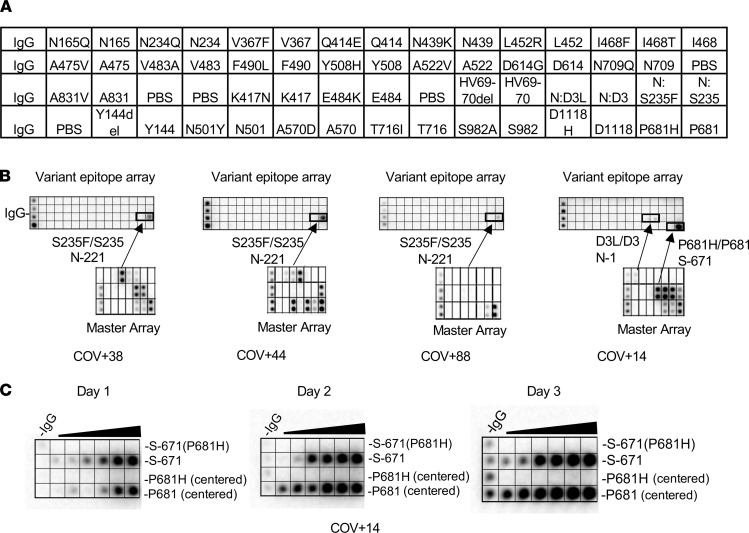
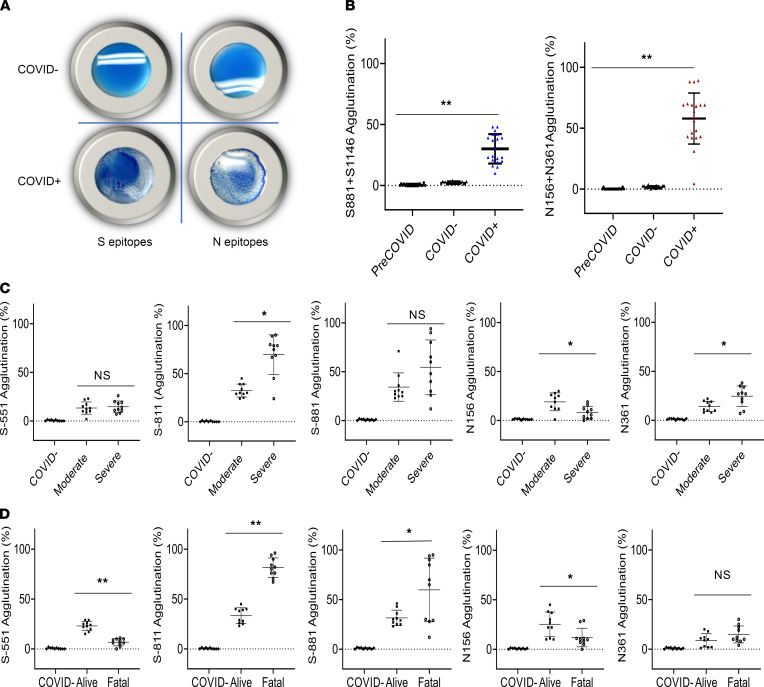
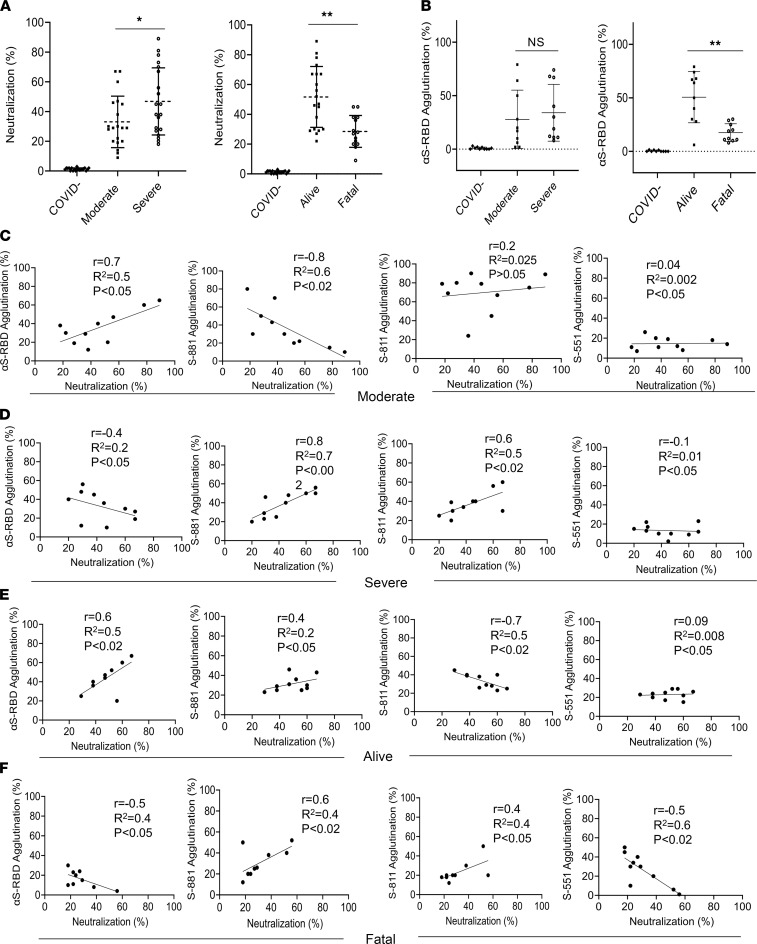
BACKGROUNDThe role of humoral immunity in COVID-19 is not fully understood, owing, in large part, to the complexity of antibodies produced in response to the SARS-CoV-2 infection. There is a pressing need for serology tests to assess patient-specific antibody response and predict clinical outcome.METHODSUsing SARS-CoV-2 proteome and peptide microarrays, we screened 146 COVID-19 patients' plasma samples to identify antigens and epitopes. This enabled us to develop a master epitope array and an epitope-specific agglutination assay to gauge antibody responses systematically and with high resolution.RESULTSWe identified linear epitopes from the spike (S) and nucleocapsid (N) proteins and showed that the epitopes enabled higher resolution antibody profiling than the S or N protein antigen. Specifically, we found that antibody responses to the S-811-825, S-881-895, and N-156-170 epitopes negatively or positively correlated with clinical severity or patient survival. Moreover, we found that the P681H and S235F mutations associated with the coronavirus variant of concern B.1.1.7 altered the specificity of the corresponding epitopes.CONCLUSIONEpitope-resolved antibody testing not only affords a high-resolution alternative to conventional immunoassays to delineate the complex humoral immunity to SARS-CoV-2 and differentiate between neutralizing and non-neutralizing antibodies, but it also may potentially be used to predict clinical outcome. The epitope peptides can be readily modified to detect antibodies against variants of concern in both the peptide array and latex agglutination formats.FUNDINGOntario Research Fund (ORF) COVID-19 Rapid Research Fund, Toronto COVID-19 Action Fund, Western University, Lawson Health Research Institute, London Health Sciences Foundation, and Academic Medical Organization of Southwestern Ontario (AMOSO) Innovation Fund.
Keywords: COVID-19; Immunoglobulins; Infectious disease.
Conflict of interest statement
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
