

Impact of Policy and Funding Decisions on COVID-19 Surveillance Operations and Case Reports - South Sudan, April 2020-February 2021
- PMID: 34081689
- PMCID: PMC8174676
- DOI: 10.15585/mmwr.mm7022a3
Impact of Policy and Funding Decisions on COVID-19 Surveillance Operations and Case Reports - South Sudan, April 2020-February 2021
Abstract
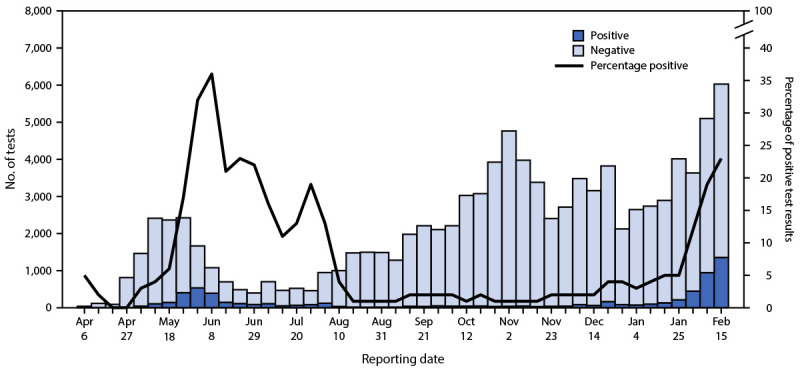
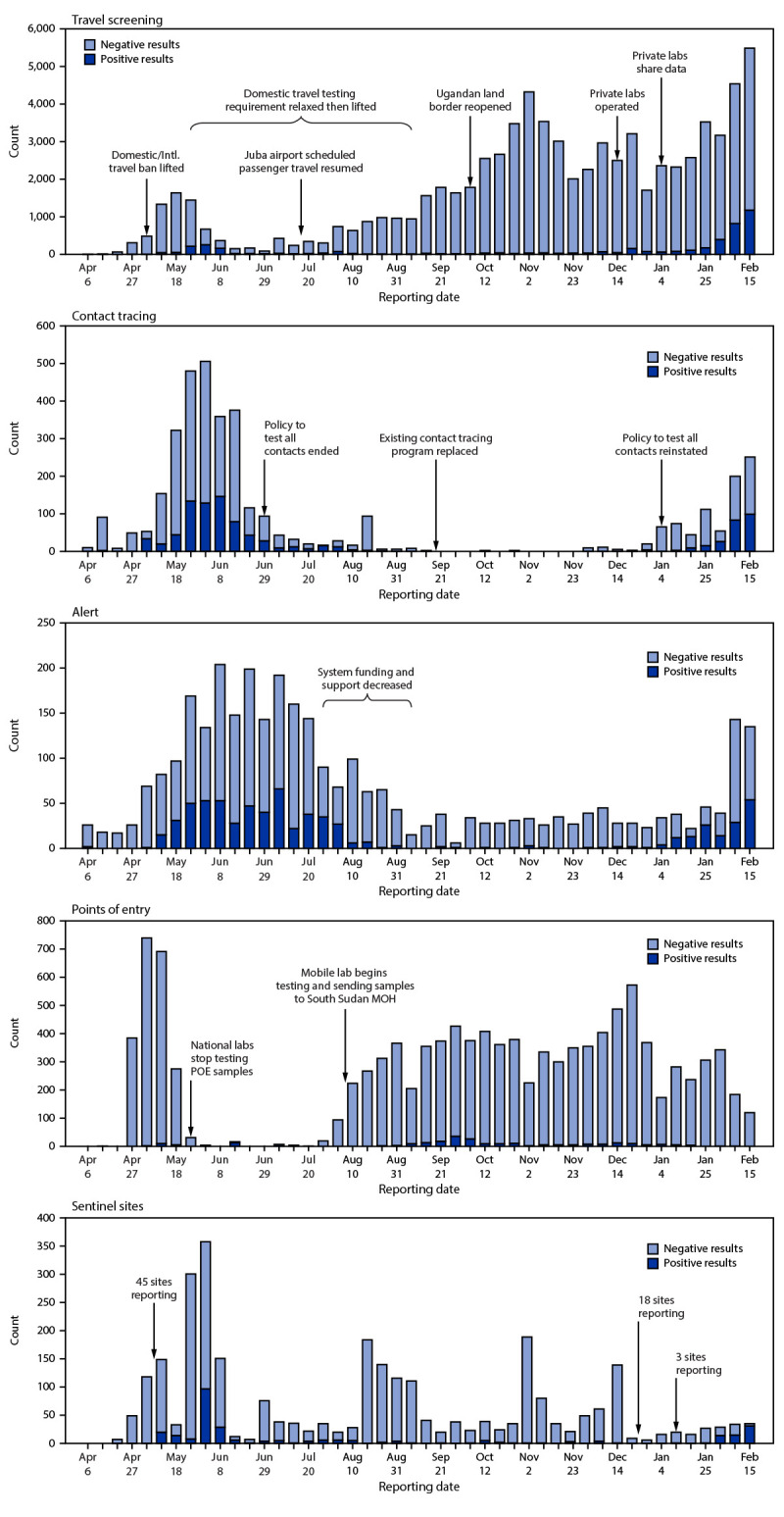
Early models predicted substantial COVID-19-associated morbidity and mortality across Africa (1-3). However, as of March 2021, countries in Africa are among those with the lowest reported incidence of COVID-19 worldwide (4). Whether this reflects effective mitigation, outbreak response, or demographic characteristics, (5) or indicates limitations in disease surveillance capacity is unclear (6). As countries implemented changes in funding, national policies, and testing strategies in response to the COVID-19 pandemic, surveillance capacity might have been adversely affected. This study assessed whether changes in surveillance operations affected reporting in South Sudan; testing and case numbers reported during April 6, 2020-February 21, 2021, were analyzed relative to the timing of funding, policy, and strategy changes.* South Sudan, with a population of approximately 11 million, began COVID-19 surveillance in February 2020 and reported 6,931 cases through February 21, 2021. Surveillance data analyzed were from point of entry screening, testing of symptomatic persons who contacted an alert hotline, contact tracing, sentinel surveillance, and outbound travel screening. After travel restrictions were relaxed in early May 2020, international land and air travel resumed and mandatory requirements for negative pretravel test results were initiated. The percentage of all testing accounted for by travel screening increased >300%, from 21.1% to 91.0% during the analysis period, despite yielding the lowest percentage of positive tests among all sources. Although testing of symptomatic persons and contact tracing yielded the highest percentage of COVID-19 cases, the percentage of all testing from these sources decreased 88%, from 52.6% to 6.3% after support for these activities was reduced. Collectively, testing increased over the project period, but shifted toward sources least likely to yield positive results, possibly resulting in underreporting of cases. Policy, funding, and strategy decisions related to the COVID-19 pandemic response, such as those implemented in South Sudan, are important issues to consider when interpreting the epidemiology of COVID-19 outbreaks.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- World Health Organization. Weekly epidemiological update–2 March 2021. Geneva, Switzerland: United Nations, World Health Organization; 2021. Accessed Mar 24, 2021. https://www.who.int/publications/m/item/weekly-epidemiological-update---...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
