

Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer
- PMID: 34081848
- PMCID: PMC9126186
- DOI: 10.1056/NEJMoa2105215
Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer
Abstract
Background: Poly(adenosine diphosphate-ribose) polymerase inhibitors target cancers with defects in homologous recombination repair by synthetic lethality. New therapies are needed to reduce recurrence in patients with BRCA1 or BRCA2 germline mutation-associated early breast cancer.
Methods: We conducted a phase 3, double-blind, randomized trial involving patients with human epidermal growth factor receptor 2 (HER2)-negative early breast cancer with BRCA1 or BRCA2 germline pathogenic or likely pathogenic variants and high-risk clinicopathological factors who had received local treatment and neoadjuvant or adjuvant chemotherapy. Patients were randomly assigned (in a 1:1 ratio) to 1 year of oral olaparib or placebo. The primary end point was invasive disease-free survival.
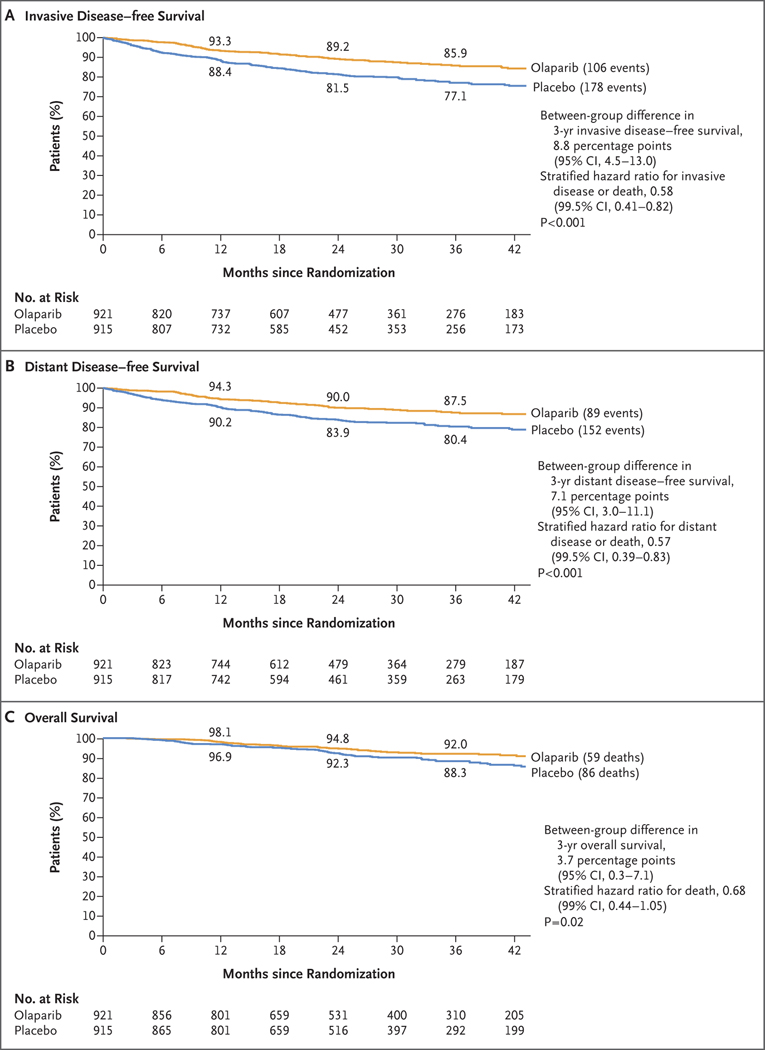
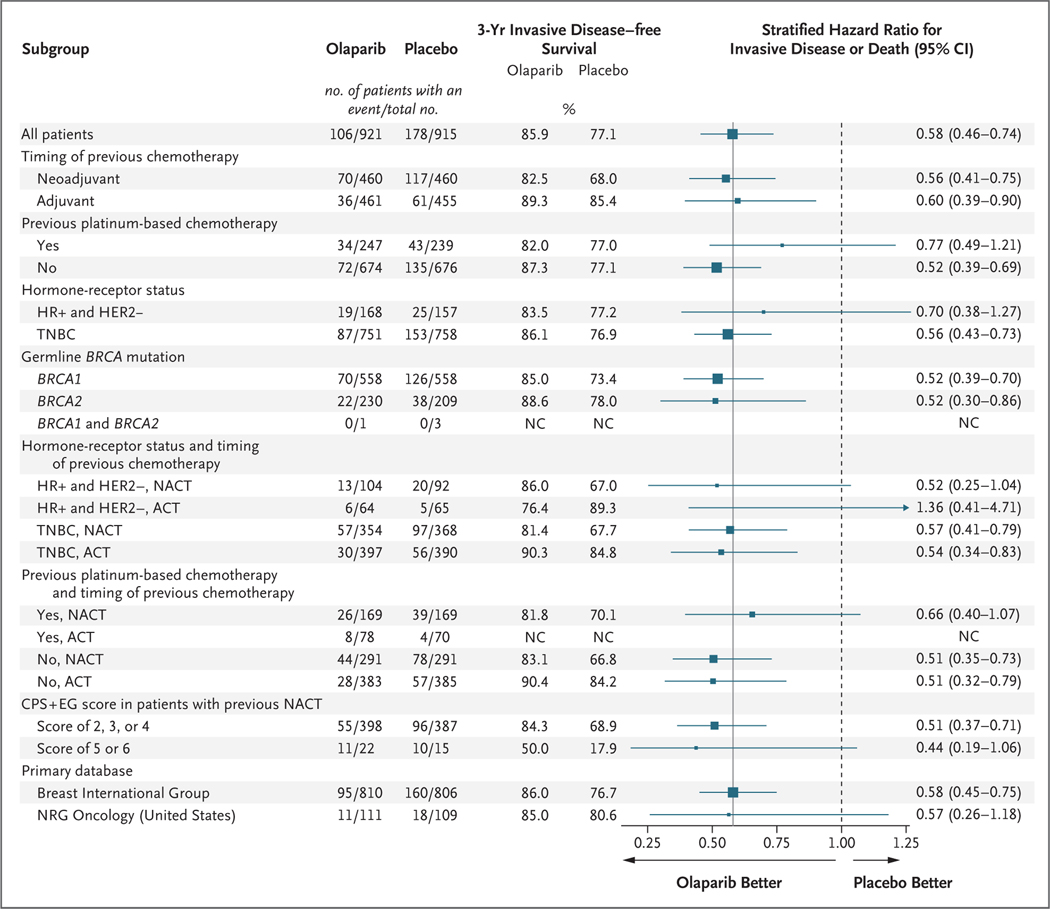
Results: A total of 1836 patients underwent randomization. At a prespecified event-driven interim analysis with a median follow-up of 2.5 years, the 3-year invasive disease-free survival was 85.9% in the olaparib group and 77.1% in the placebo group (difference, 8.8 percentage points; 95% confidence interval [CI], 4.5 to 13.0; hazard ratio for invasive disease or death, 0.58; 99.5% CI, 0.41 to 0.82; P<0.001). The 3-year distant disease-free survival was 87.5% in the olaparib group and 80.4% in the placebo group (difference, 7.1 percentage points; 95% CI, 3.0 to 11.1; hazard ratio for distant disease or death, 0.57; 99.5% CI, 0.39 to 0.83; P<0.001). Olaparib was associated with fewer deaths than placebo (59 and 86, respectively) (hazard ratio, 0.68; 99% CI, 0.44 to 1.05; P = 0.02); however, the between-group difference was not significant at an interim-analysis boundary of a P value of less than 0.01. Safety data were consistent with known side effects of olaparib, with no excess serious adverse events or adverse events of special interest.
Conclusions: Among patients with high-risk, HER2-negative early breast cancer and germline BRCA1 or BRCA2 pathogenic or likely pathogenic variants, adjuvant olaparib after completion of local treatment and neoadjuvant or adjuvant chemotherapy was associated with significantly longer survival free of invasive or distant disease than was placebo. Olaparib had limited effects on global patient-reported quality of life. (Funded by the National Cancer Institute and AstraZeneca; OlympiA ClinicalTrials.gov number, NCT02032823.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Adjuvant olaparib - should all patients with breast cancer have genetic testing?Nat Rev Clin Oncol. 2021 Oct;18(10):607-608. doi: 10.1038/s41571-021-00544-7. Nat Rev Clin Oncol. 2021. PMID: 34282304 No abstract available.
-
Adjuvant Olaparib in BRCA-Mutated Breast Cancer.N Engl J Med. 2021 Oct 7;385(15):1439. doi: 10.1056/NEJMc2112373. N Engl J Med. 2021. PMID: 34614336 No abstract available.
-
Adjuvant Olaparib in BRCA-Mutated Breast Cancer.N Engl J Med. 2021 Oct 7;385(15):1439-1440. doi: 10.1056/NEJMc2112373. N Engl J Med. 2021. PMID: 34614337 No abstract available.
References
-
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 2017; 317: 2402–16. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous