

Transcriptomics of bronchoalveolar lavage cells identifies new molecular endotypes of sarcoidosis
- PMID: 34083402
- PMCID: PMC9759791
- DOI: 10.1183/13993003.02950-2020
Transcriptomics of bronchoalveolar lavage cells identifies new molecular endotypes of sarcoidosis
Abstract
Background: Sarcoidosis is a multisystem granulomatous disease of unknown origin with a variable and often unpredictable course and pattern of organ involvement. In this study we sought to identify specific bronchoalveolar lavage (BAL) cell gene expression patterns indicative of distinct disease phenotypic traits.
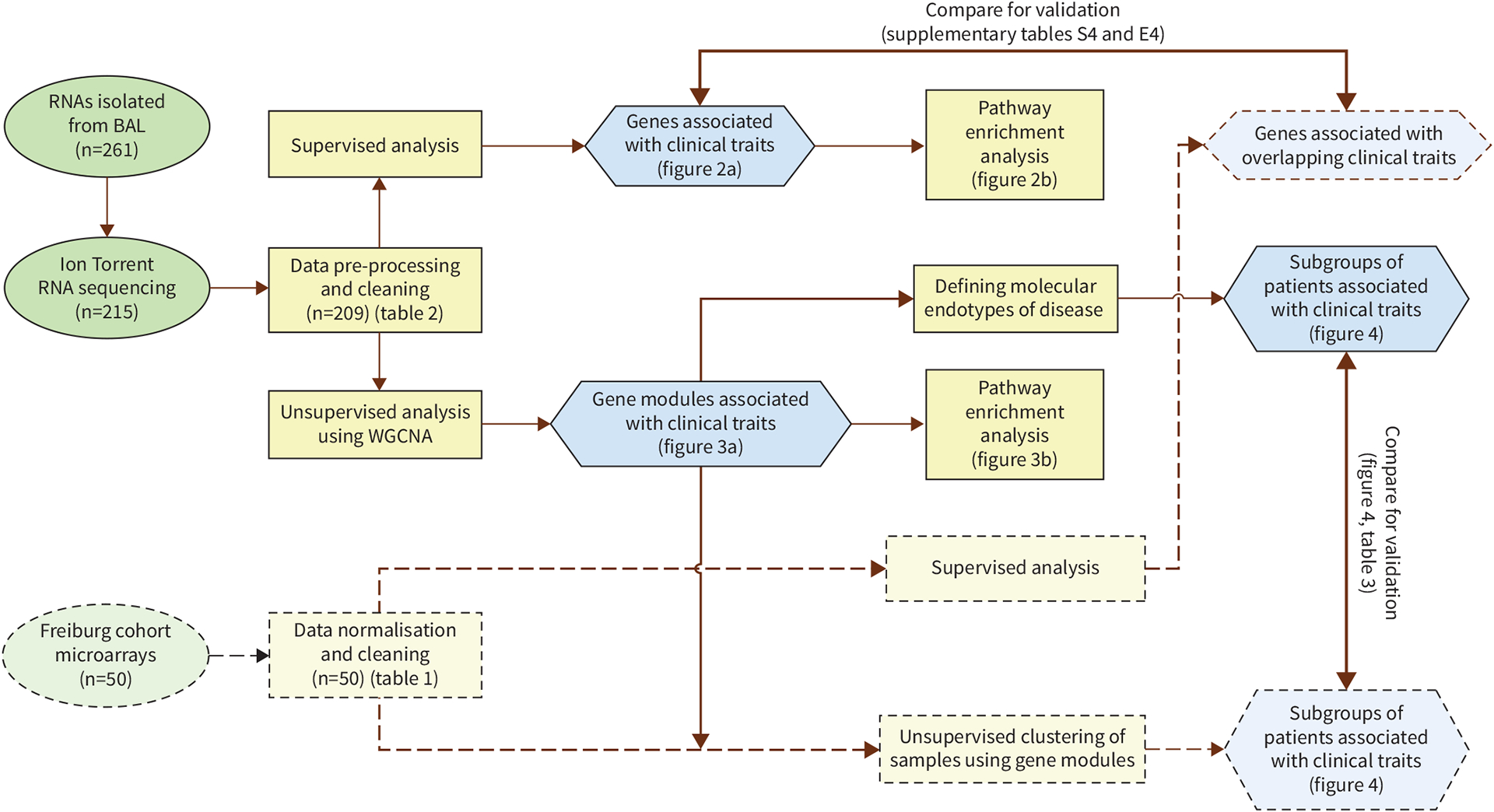
Methods: RNA sequencing by Ion Torrent Proton was performed on BAL cells obtained from 215 well-characterised patients with pulmonary sarcoidosis enrolled in the multicentre Genomic Research in Alpha-1 Antitrypsin Deficiency and Sarcoidosis (GRADS) study. Weighted gene co-expression network analysis and nonparametric statistics were used to analyse genome-wide BAL transcriptome. Validation of results was performed using a microarray expression dataset of an independent sarcoidosis cohort (Freiburg, Germany; n=50).
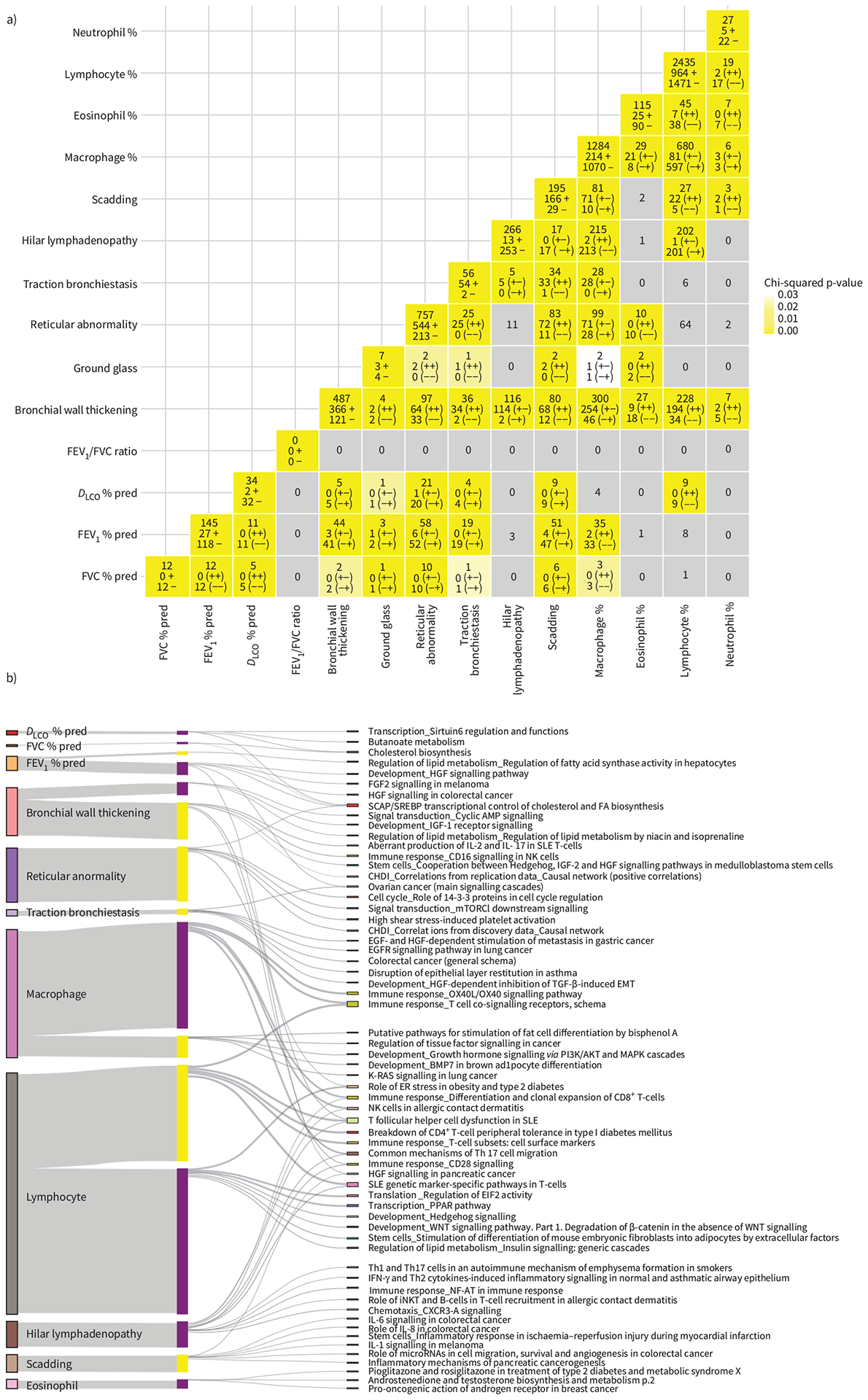
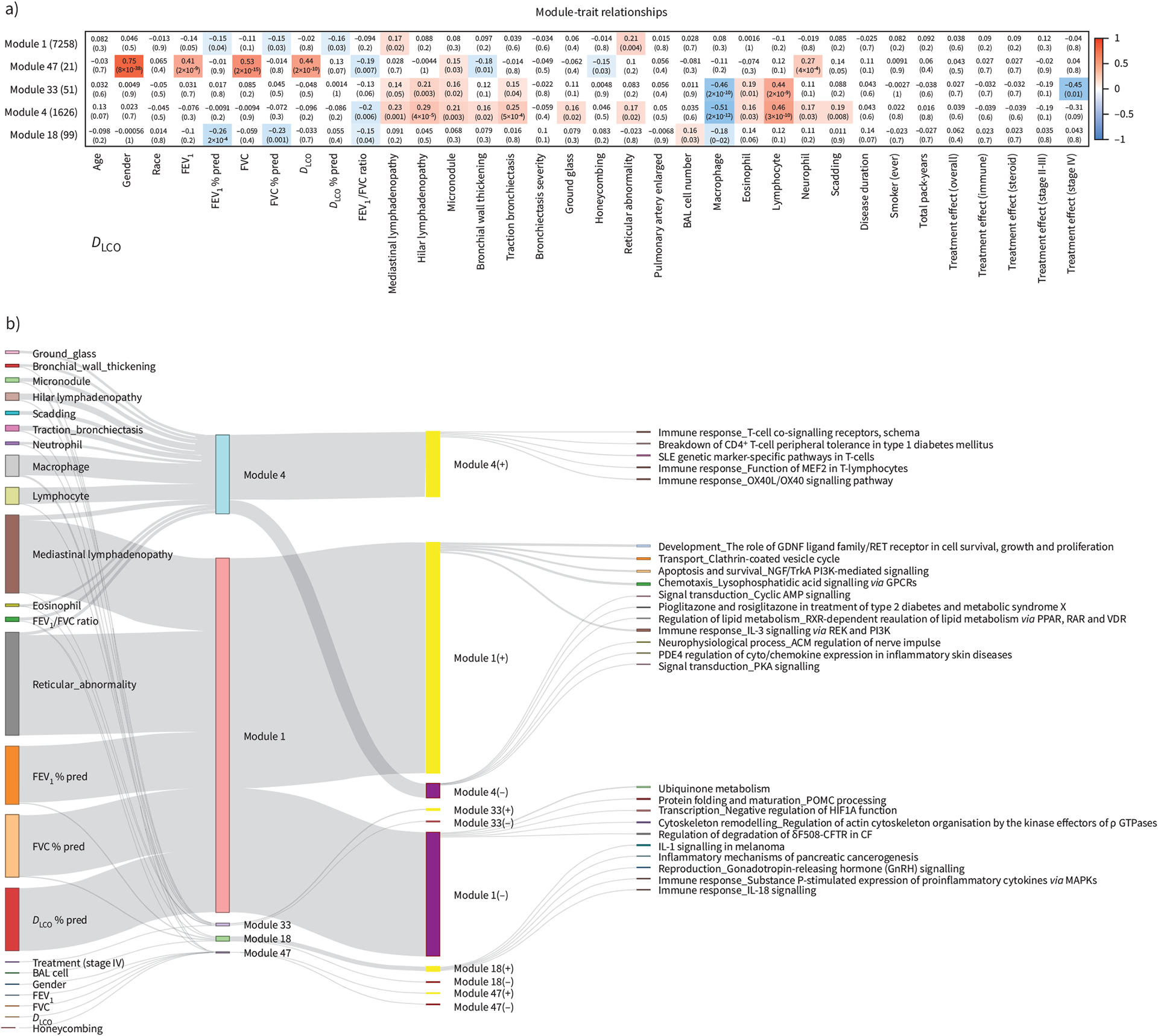
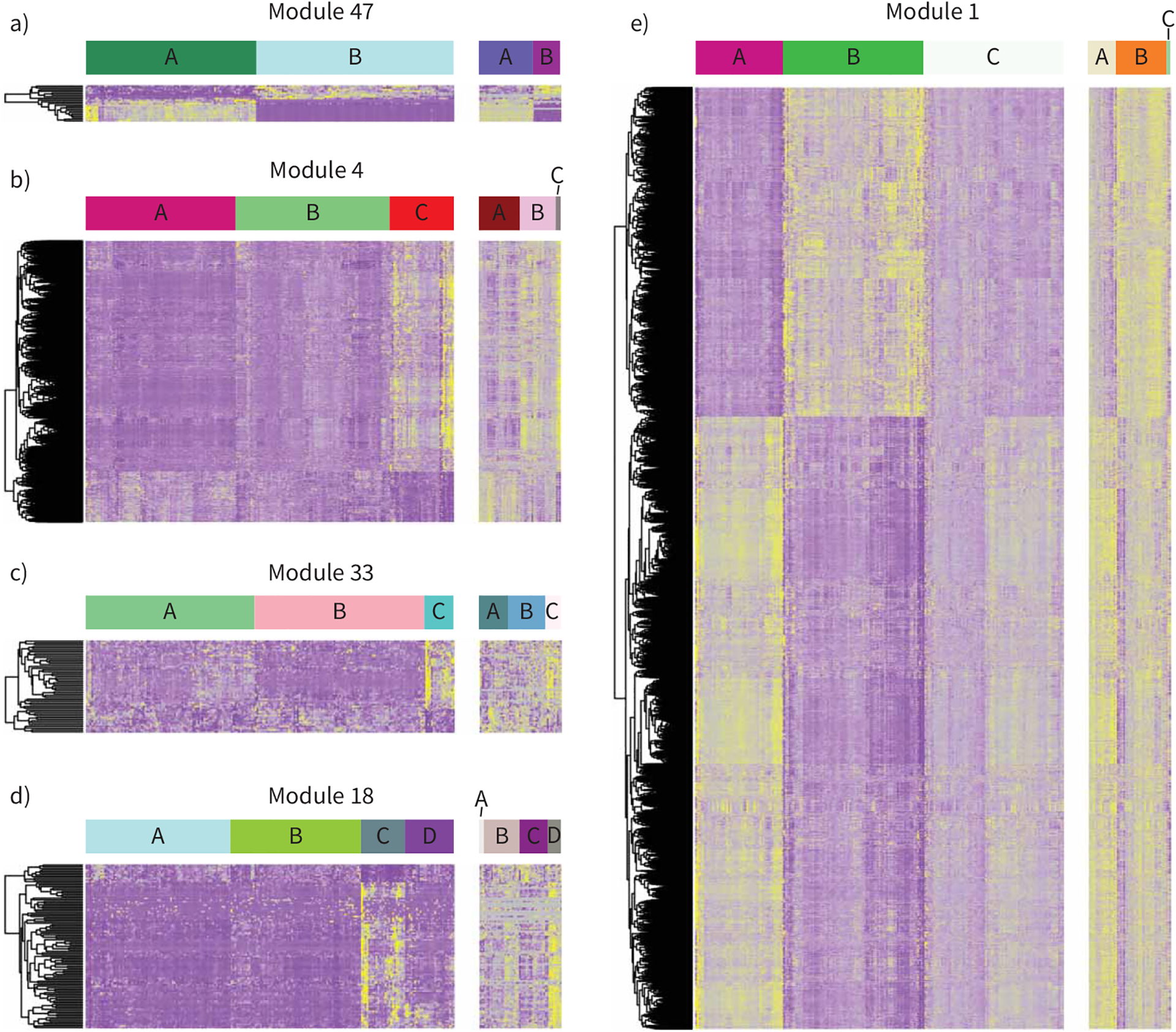
Results: Our supervised analysis found associations between distinct transcriptional programmes and major pulmonary phenotypic manifestations of sarcoidosis including T-helper type 1 (Th1) and Th17 pathways associated with hilar lymphadenopathy, transforming growth factor-β1 (TGFB1) and mechanistic target of rapamycin (MTOR) signalling with parenchymal involvement, and interleukin (IL)-7 and IL-2 with airway involvement. Our unsupervised analysis revealed gene modules that uncovered four potential sarcoidosis endotypes including hilar lymphadenopathy with increased acute T-cell immune response; extraocular organ involvement with PI3K activation pathways; chronic and multiorgan disease with increased immune response pathways; and multiorgan involvement, with increased IL-1 and IL-18 immune and inflammatory responses. We validated the occurrence of these endotypes using gene expression, pulmonary function tests and cell differentials from Freiburg.
Conclusion: Taken together, our results identify BAL gene expression programmes that characterise major pulmonary sarcoidosis phenotypes and suggest the presence of distinct disease molecular endotypes.
Copyright ©The authors 2021. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: M. Vukmirovic has nothing to disclose. Conflict of interest: X. Yan has nothing to disclose. Conflict of interest: K.F. Gibson has nothing to disclose. Conflict of interest: M. Gulati reports grants from NIH, during the conduct of the study; personal fees for advisory board work and other (PI/publication committee) from Boehringer Ingelheim, other (lectures) from France Foundation, other (PI/centre director) from Pulmonary Fibrosis Foundation, grants from NIH and Sarcoidosis Research Foundation, outside the submitted work. Conflict of interest: J.C. Schupp has nothing to disclose. Conflict of interest: G. DeIuliis has nothing to disclose. Conflict of interest: T.S. Adams has nothing to disclose. Conflict of interest: B. Hu has nothing to disclose. Conflict of interest: A. Mihaljinec has nothing to disclose. Conflict of interest: T.N. Woolard has nothing to disclose. Conflict of interest: H. Lynn has nothing to disclose. Conflict of interest: N. Emeagwali has nothing to disclose. Conflict of interest: E.L Herzog reports grants from NIH, Sanofi, Bristol Myers and Promedior, personal fees for consultancy from Boehringer Ingelheim and Pfizer, outside the submitted work. Conflict of interest: E.S. Chen has nothing to disclose. Conflict of interest: A. Morris reports grants from NIH, during the conduct of the study. Conflict of interest: J.K. Leader has nothing to disclose. Conflict of interest: Y. Zhang has nothing to disclose. Conflict of interest: J.G.N. Garcia has nothing to disclose. Conflict of interest: L.A. Maier grants from NIH (1U01 HL112695-01, U01 HL112707-03) and NIH/NCRR (UL1TRR002535), during the conduct of the study; grants from National Institutes of Health (1R01 HL127461-01A1, R01HL136681-01A1, 1R01 HL140357-01A1, R01HL136681-01A1), FSR, University of Cinncinati under a Mallinckrodt foundation, MNK14344100, ATYR1923-C-002, outside the submitted work; and is a member of the FSR scientific advisory board, for which no compensation is received. Conflict of interest: R.G. Collman reports grants from National Institutes of Health, during the conduct of the study. Conflict of interest: W.P. Drake has nothing to disclose. Conflict of interest: M.J. Becich reports grants from NCATS, NCI, PCORI, NHLBI and CDC NIOSH, other (startup) from SpIntellx, during the conduct of the study; other (startup) from SpIntellx, outside the submitted work; and has patents SpIntellx (multiple) pending. Conflict of interest: H. Hochheiser has nothing to disclose. Conflict of interest: S.R. Wisniewski has nothing to disclose. Conflict of interest: P.V. Benos has nothing to disclose. Conflict of interest: D.R. Moller reports grants from NHLBI (1U01HL112708), during the conduct of the study; personal fees for consultancy from Merck, aTYR and Roivant, personal fees for advisory board work from SarcoMed, personal fees for consultancy/witness from Legal Expert, other (royalties) from Hodder Education and Taylor & Francis Group, outside the submitted work; has patents number 9,683,999 B2 issued, and number 9,977,029 B2 issued; is Chairman and Chief Technical Officer of Sarcoidosis Diagnostic Testing, LLC (a company whose goal is to develop a diagnostic blood test for sarcoidosis) and has received funding including past salary support under the NHLBI STTR programme, grant R41 HL129728 more than 3 years ago; and is a former member of the Scientific Advisory Board of the Foundation for Sarcoidosis Research. Conflict of interest: A. Prasse reports personal fees for lectures and consultancy and non-financial support for meeting attendance from Boehringer Ingelheim and Roche, personal fees for lectures from Novartis and AstraZeneca, personal fees for consultancy from Amgen, Pliant and Nitto Denko, outside the submitted work. Conflict of interest: L.L. Koth has nothing to disclose. Conflict of interest: N. Kaminski reports personal fees for consultancy and/or advisory board work from Biogen Idec, Boehringer Ingelheim, Third Rock, Samumed, NuMedii, Indaloo, Theravance, LifeMax, Three Lake Partners, RohBar and Pliant, non-financial support from Miragen, equity with Pliant, a grant from Veracyte; all outside the submitted work; and has a patent New Therapies in Pulmonary Fibrosis and on Peripheral Blood Gene Expression that have been licensed to Biotech.
Figures
References
-
- Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med 1999; 160: 736–755. - PubMed
-
- Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med 2007; 357: 2153–2165. - PubMed
-
- Baughman RP, Costabel U, du Bois RM. Treatment of sarcoidosis. Clin Chest Med 2008; 29: 533–548. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL112694/HL/NHLBI NIH HHS/United States
- R01 HL140357/HL/NHLBI NIH HHS/United States
- U01 HL112711/HL/NHLBI NIH HHS/United States
- R01 HL127349/HL/NHLBI NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- R01 HL110883/HL/NHLBI NIH HHS/United States
- U24OH009077/ACL/ACL HHS/United States
- U01 HL112707/HL/NHLBI NIH HHS/United States
- U01 HL112702/HL/NHLBI NIH HHS/United States
- U01 HL112695/HL/NHLBI NIH HHS/United States
- U24 OH009077/OH/NIOSH CDC HHS/United States
- UL1 RR029882/RR/NCRR NIH HHS/United States
- R56 HL149129/HL/NHLBI NIH HHS/United States
- U01 HL112696/HL/NHLBI NIH HHS/United States
- U01 HL112712/HL/NHLBI NIH HHS/United States
- U01 HL137159/HL/NHLBI NIH HHS/United States
- R01 HL127461/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- U01 HL112708/HL/NHLBI NIH HHS/United States
- R21 LM012884/LM/NLM NIH HHS/United States
- R01 HL136681/HL/NHLBI NIH HHS/United States
- R41 HL129728/HL/NHLBI NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- R01 HL114587/HL/NHLBI NIH HHS/United States
- R01 HL117074/HL/NHLBI NIH HHS/United States
- K24 HL127301/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous