

Comparative study on clinical efficacy of different methods for the treatment of intramural aortic hematoma
- PMID: 34083629
- PMCID: PMC8175714
- DOI: 10.1038/s41598-021-91151-0
Comparative study on clinical efficacy of different methods for the treatment of intramural aortic hematoma
Abstract
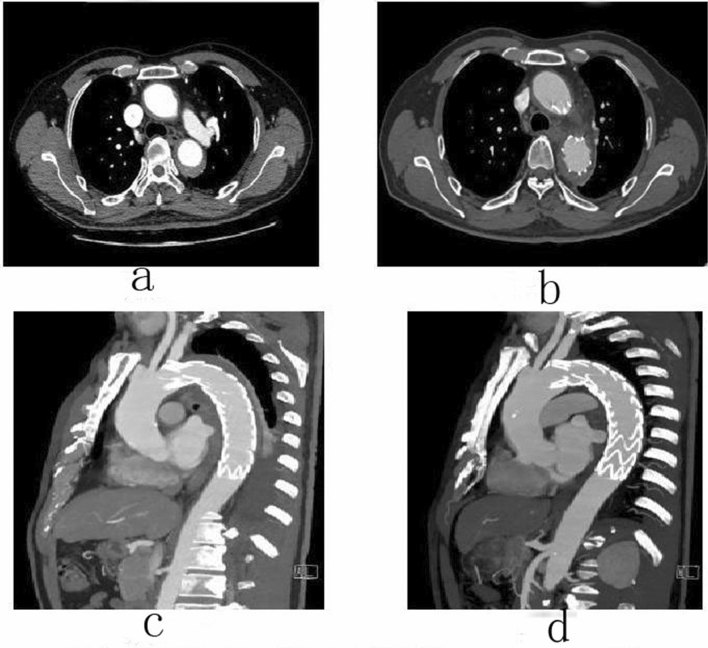
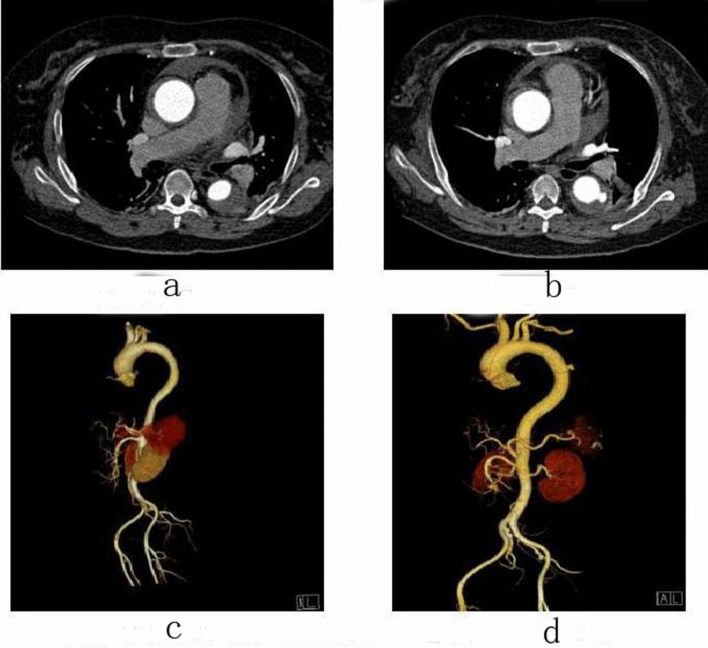
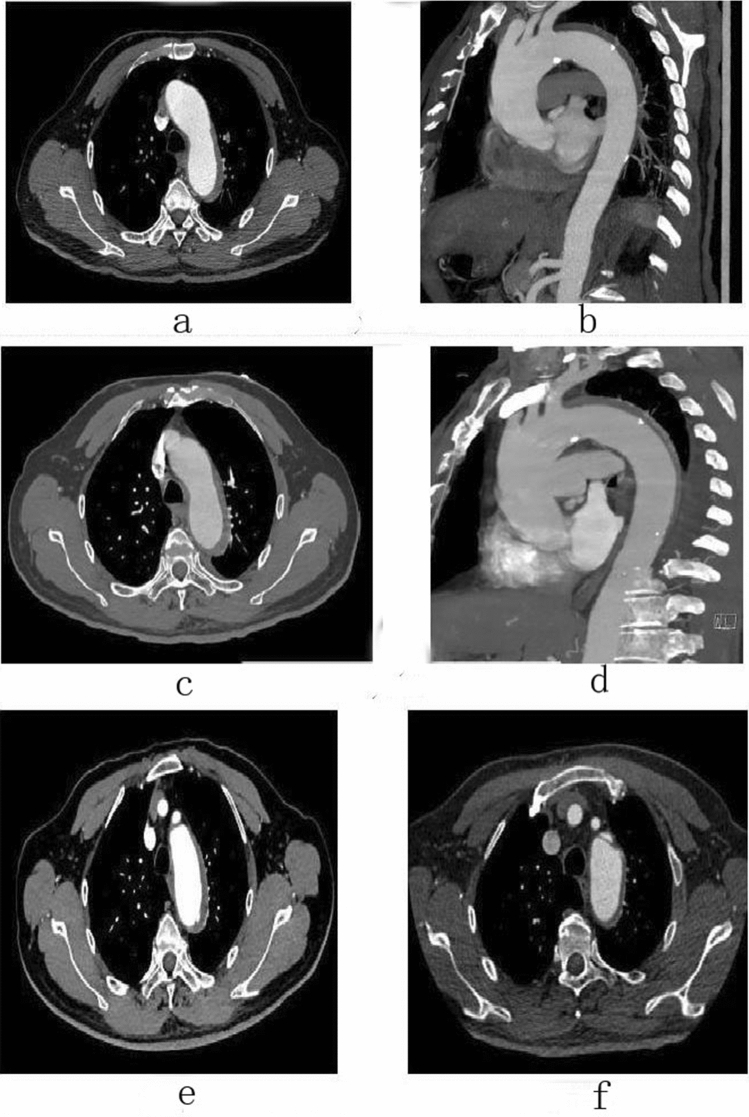
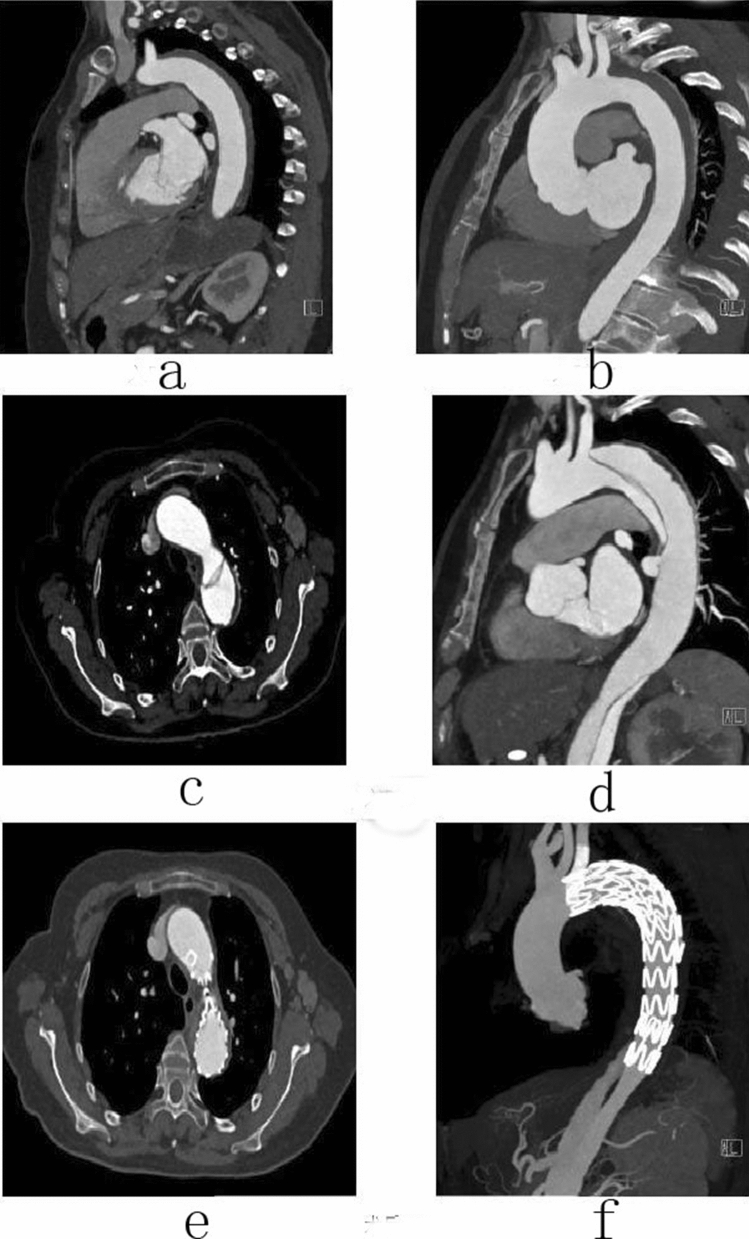
To explore the difference of curative effect between different treatment modalities, in order to provide reference for the treatment of aortic intramural hematoma (IMH). 168 patients with aortic intramural hematoma diagnosed and treated from January 2010 to July 2020 were selected in the Second Affiliated Hospital of Nanchang University. Among them, 48 patients were diagnosed with Stanford A aortic intramural hematoma and 120 were diagnosed with Stanford B aortic intramural hematoma. According to the therapeutic methods, patients were divided into conservative treatment group and endovascular treatment group (TEVAR). For endovascular treatment group, according to the different timing of surgery, can be divided into acute phase group (onset within 72 h) and non-acute phase group (time of onset > 72 h).The clinical data and follow-up data were collected and analyzed by variance analysis and χ2 test. There were 168 patients diagnosed with aortic intramural hematoma 39 of them were (81.25%) Stanford A aortic intramural hematoma patients with pleural or pericardial effusion. For patient with Stanford A aortic intramural hematoma, endovascular treatment was performed in 15 patients (31.2%), and 33 cases (68.8%) for conservative treatment. The average follow-up (24.9 ± 13.9) was months. There were 120 patients with Stanford type B aortic intramural hematoma (71.4%), 60 patients received endovascular treatment (50%), and 60 patients (50%) received conservative treatment, with an average follow-up of (27.8 ± 14.6) months. For Stanford A type aortic intramural hematoma patients when the maximum aortic diameter ≥ 50 mm or hematoma thickness ≥ 11 mm, with high morbidity and mortality, positive endovascular treatment can reduce complications and death. For patients with Stanford type B aortic intramural hematoma, when the maximum aortic diameter ≥ 40 mm or hematoma thickness ≥ 10 mm, with high morbidity and mortality, positive endovascular treatment can reduce complications and death. Both Stanford type A and B aortic intramural hematoma patients could benefit from the endovascular treatment when the initial maximum aortic diameter is ≥ 50 mm or the hematoma thickness is ≥ 11 mm.
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Outcome After Conservative and Endovascular Treatment of Stanford Type B Aortic Intramural Hematomas - A Single-Center Retrospective Study.Vasc Endovascular Surg. 2024 Jul;58(5):477-485. doi: 10.1177/15385744231225888. Epub 2023 Dec 29. Vasc Endovascular Surg. 2024. PMID: 38157519 Free PMC article.
-
Long-term behavior of aortic intramural hematomas and penetrating ulcers.J Thorac Cardiovasc Surg. 2016 Feb;151(2):361-72, 373.e1. doi: 10.1016/j.jtcvs.2015.09.012. Epub 2015 Sep 16. J Thorac Cardiovasc Surg. 2016. PMID: 26496809
-
Impact of thoracic endovascular aortic repair timing on aortic remodeling in acute type B aortic intramural hematoma.J Vasc Surg. 2022 Feb;75(2):464-472.e2. doi: 10.1016/j.jvs.2021.08.059. Epub 2021 Sep 8. J Vasc Surg. 2022. PMID: 34506888
-
Thoracic Endovascular Aortic Repair versus Best Medical Treatment for High-Risk Type B Intramural Hematoma: A Systematic Review of Clinical Studies.Ann Vasc Surg. 2018 Oct;52:273-279. doi: 10.1016/j.avsg.2018.03.010. Epub 2018 May 22. Ann Vasc Surg. 2018. PMID: 29793011
-
Diagnosis and management of acute aortic syndromes: dissection, intramural hematoma, and penetrating aortic ulcer.Curr Cardiol Rep. 2014;16(10):536. doi: 10.1007/s11886-014-0536-x. Curr Cardiol Rep. 2014. PMID: 25156302 Review.
Cited by
-
Potential biomarkers of aortic dissection based on expression network analysis.BMC Cardiovasc Disord. 2023 Mar 23;23(1):147. doi: 10.1186/s12872-023-03173-3. BMC Cardiovasc Disord. 2023. PMID: 36959563 Free PMC article.
-
Outcome After Conservative and Endovascular Treatment of Stanford Type B Aortic Intramural Hematomas - A Single-Center Retrospective Study.Vasc Endovascular Surg. 2024 Jul;58(5):477-485. doi: 10.1177/15385744231225888. Epub 2023 Dec 29. Vasc Endovascular Surg. 2024. PMID: 38157519 Free PMC article.
-
Thoracic Endovascular Aortic Repair versus Optimal Medical Treatment in Patients with Type B Intramural Hematoma: A Meta-Analysis.Ann Thorac Cardiovasc Surg. 2023 Aug 20;29(4):177-184. doi: 10.5761/atcs.ra.22-00219. Epub 2023 Feb 16. Ann Thorac Cardiovasc Surg. 2023. PMID: 36792204 Free PMC article.
References
-
- Mir J, Peihua Z. Clinical Vasopulmonary Surgery 3. Science Press; 2011. pp. 324–325.
-
- Cronenwett JL, Wayne Johnston K. Rutherford’s Vascular Surgery. Saunders; 2014. pp. 2186–2188.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
