

Lung microbiome alterations in NSCLC patients
- PMID: 34083661
- PMCID: PMC8175694
- DOI: 10.1038/s41598-021-91195-2
Lung microbiome alterations in NSCLC patients
Abstract
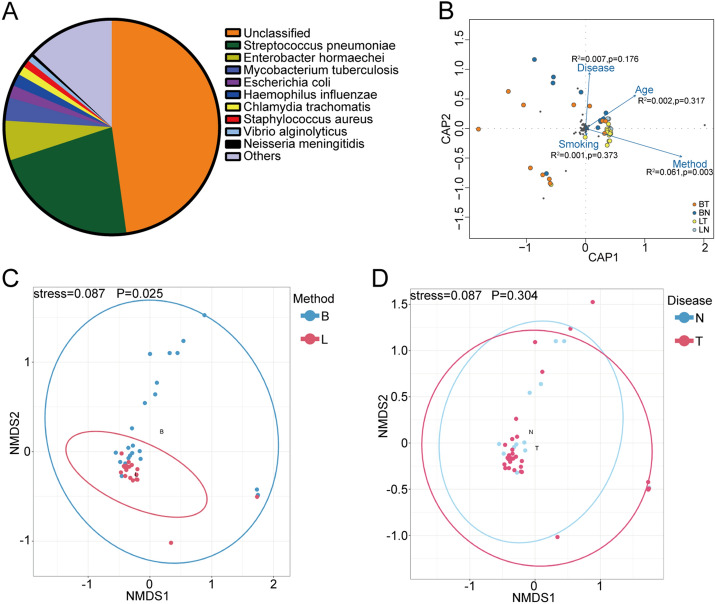
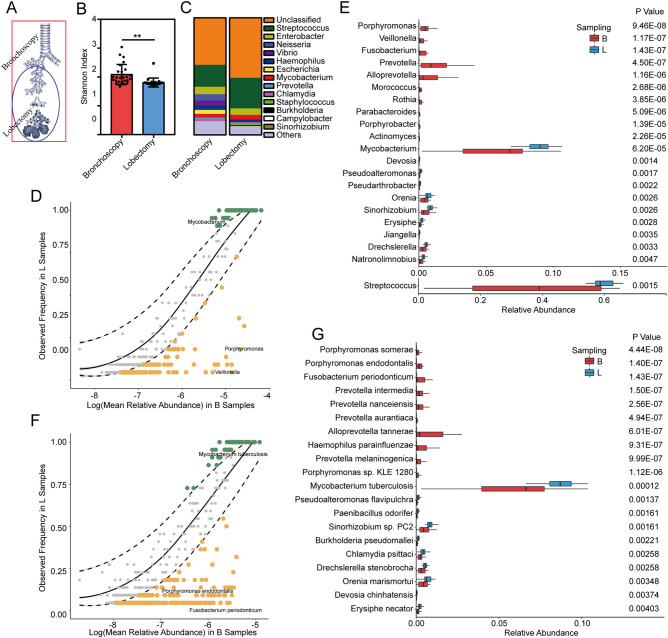
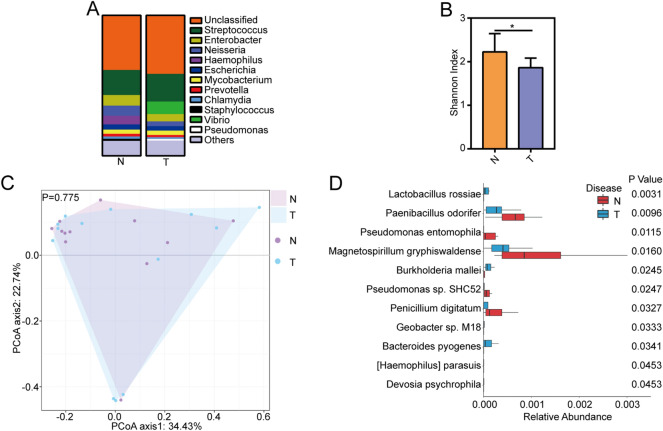
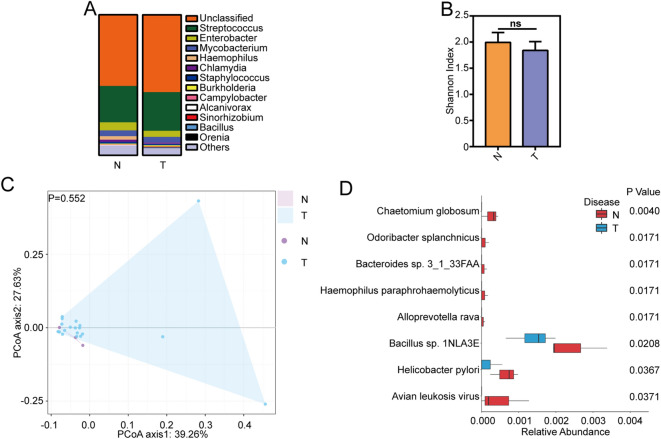
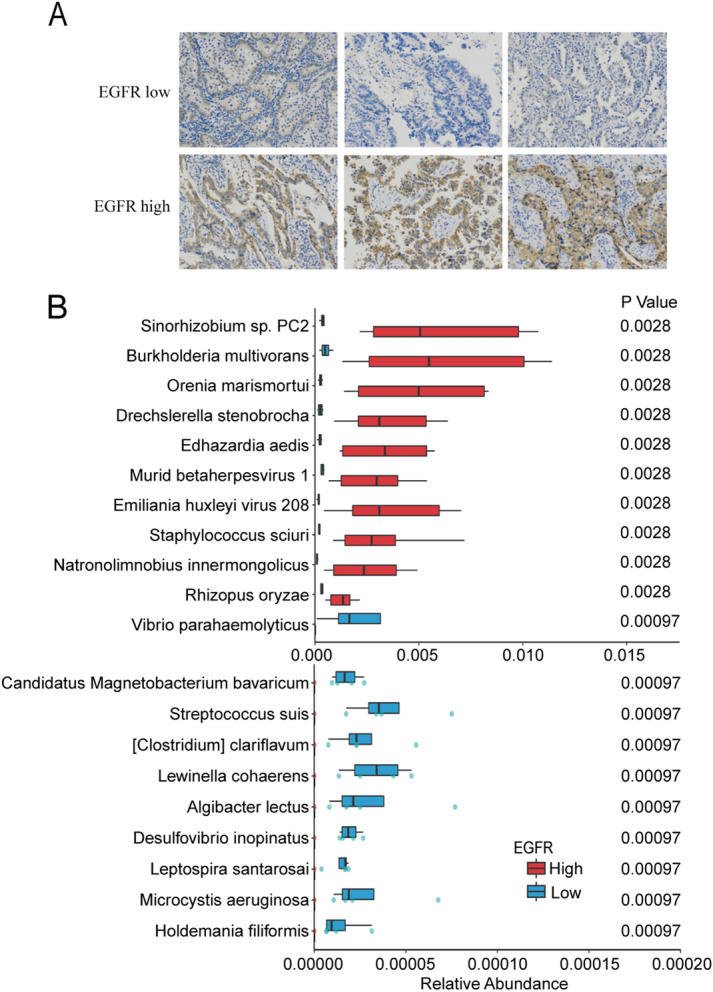
Lung is colonized by a diverse array of microbes and the lung microbiota is profoundly involved in the development of respiratory diseases. There is little knowledge about the role of lung microbiota dysbiosis in lung cancer. In this study, we performed metagenomic sequencing on bronchoalveolar lavage (BAL) from two different sampling methods in non-small cell lung cancer (NSCLC) patients and non-cancer controls. We found the obvious variation between bronchoscopy samples and lobectomy samples. Oral taxa can be found in both bronchoscopy and lobectomy samples and higher abundance of oral taxa can be found in bronchoscopy samples. Although the NSCLC patients had similar microbial communities with non-cancer controls, rare species such as Lactobacillus rossiae, Bacteroides pyogenes, Paenibacillus odorifer, Pseudomonas entomophila, Magnetospirillum gryphiswaldense, fungus Chaetomium globosum et al. showed obvious difference between NSCLC patients and non-cancer controls. Age-, gender-, and smoking-specific species and EGFR expression-related species in NSCLC patients were detected. There results implicated that different lung segments have differential lung microbiome composition. The oral taxa are found in the lobectomy samples suggesting that oral microbiota are the true members of lung microbiota, rather than contamination during bronchoscopy. Lung cancer does not obviously alter the global microbial composition, while rare species are altered more than common species. Certain microbes may be associated with lung cancer progression.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Alterations of the Human Lung and Gut Microbiomes in Non-Small Cell Lung Carcinomas and Distant Metastasis.Microbiol Spectr. 2021 Dec 22;9(3):e0080221. doi: 10.1128/Spectrum.00802-21. Epub 2021 Nov 17. Microbiol Spectr. 2021. PMID: 34787462 Free PMC article.
-
Dysbiosis of lower respiratory tract microbiome are associated with inflammation and microbial function variety.Respir Res. 2019 Dec 3;20(1):272. doi: 10.1186/s12931-019-1246-0. Respir Res. 2019. PMID: 31796027 Free PMC article.
-
Metagenomics and Non-Targeted Metabolomics Reveal the Role of Gut Microbiota and Its Metabolites in Brain Metastasis of Non-Small Cell Lung Cancer.Thorac Cancer. 2025 Apr;16(8):e70068. doi: 10.1111/1759-7714.70068. Thorac Cancer. 2025. PMID: 40263747 Free PMC article.
-
Symbiotic microbial communities in various locations of the lung cancer respiratory tract along with potential host immunological processes affected.Front Cell Infect Microbiol. 2024 Feb 2;14:1296295. doi: 10.3389/fcimb.2024.1296295. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38371298 Free PMC article. Review.
-
Microbial biomarker development for detection and prognosis of early-stage non-small cell lung cancer.Cancer Biomark. 2025 Apr;42(4):18758592251322045. doi: 10.1177/18758592251322045. Epub 2025 Apr 29. Cancer Biomark. 2025. PMID: 40302376 Review.
Cited by
-
One-step diagnosis of infection and lung cancer using metagenomic sequencing.Respir Res. 2025 Feb 4;26(1):48. doi: 10.1186/s12931-025-03127-7. Respir Res. 2025. PMID: 39905469 Free PMC article.
-
Exploring the microbiome: Uncovering the link with lung cancer and implications for diagnosis and treatment.Chin Med J Pulm Crit Care Med. 2023 Sep 15;1(3):161-170. doi: 10.1016/j.pccm.2023.08.003. eCollection 2023 Sep. Chin Med J Pulm Crit Care Med. 2023. PMID: 39171127 Free PMC article. Review.
-
The Complex Role of the Microbiome in Non-Small Cell Lung Cancer Development and Progression.Cells. 2023 Dec 8;12(24):2801. doi: 10.3390/cells12242801. Cells. 2023. PMID: 38132121 Free PMC article. Review.
-
The lung, the niche, and the microbe: Exploring the lung microbiome in cancer and immunity.Front Immunol. 2023 Jan 17;13:1094110. doi: 10.3389/fimmu.2022.1094110. eCollection 2022. Front Immunol. 2023. PMID: 36733391 Free PMC article. Review.
-
Alterations of the Human Lung and Gut Microbiomes in Non-Small Cell Lung Carcinomas and Distant Metastasis.Microbiol Spectr. 2021 Dec 22;9(3):e0080221. doi: 10.1128/Spectrum.00802-21. Epub 2021 Nov 17. Microbiol Spectr. 2021. PMID: 34787462 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
