

Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018
- PMID: 34083753
- PMCID: PMC8373614
- DOI: 10.1038/s41562-021-01108-6
Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018
Abstract
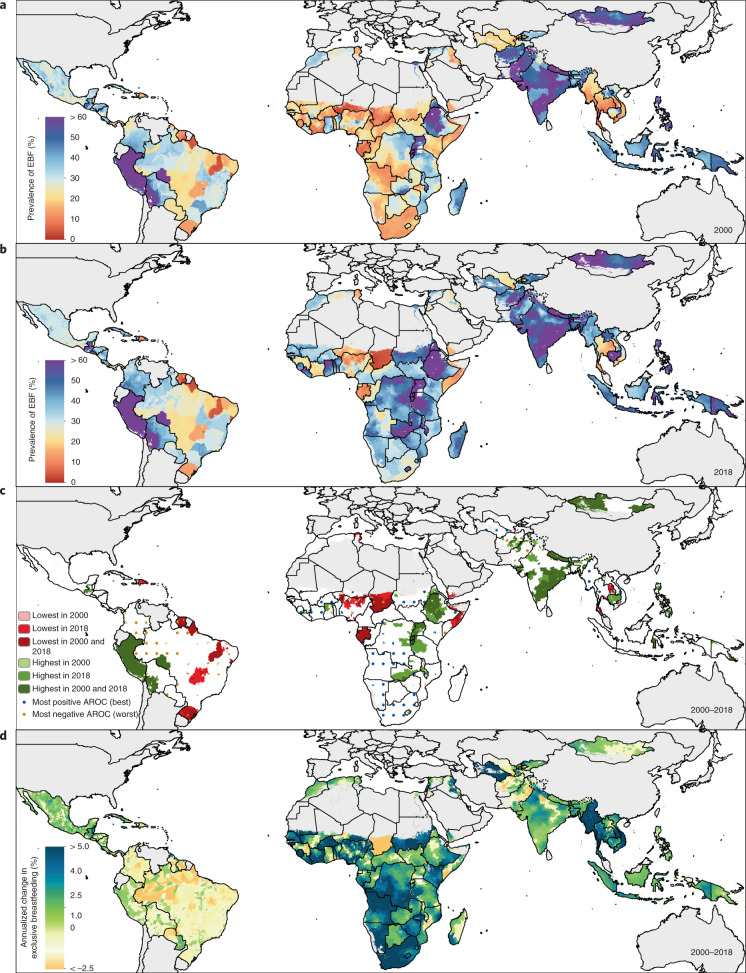
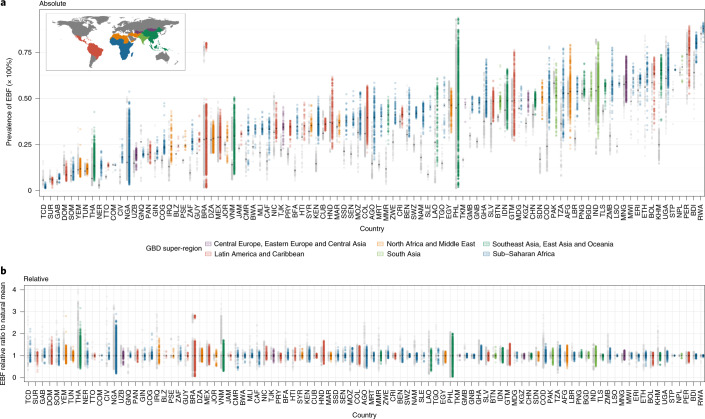
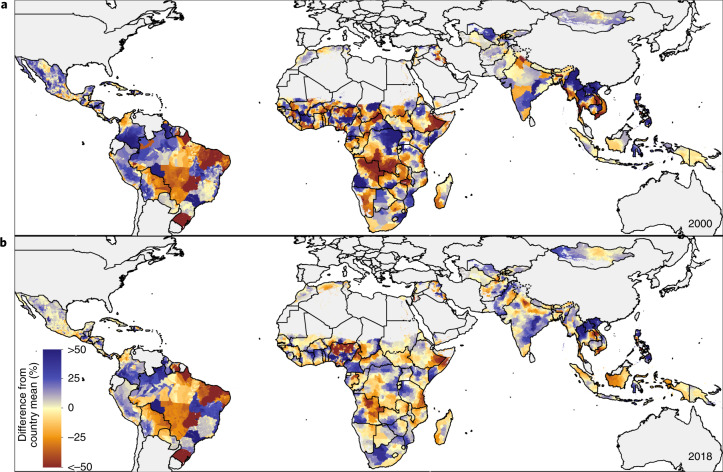
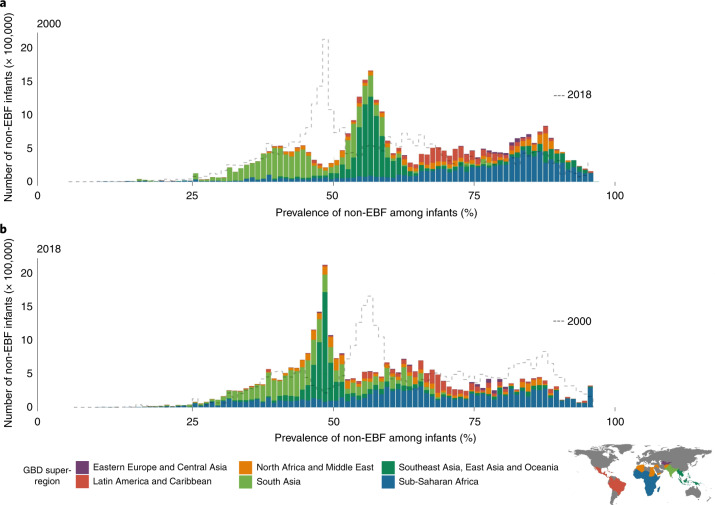
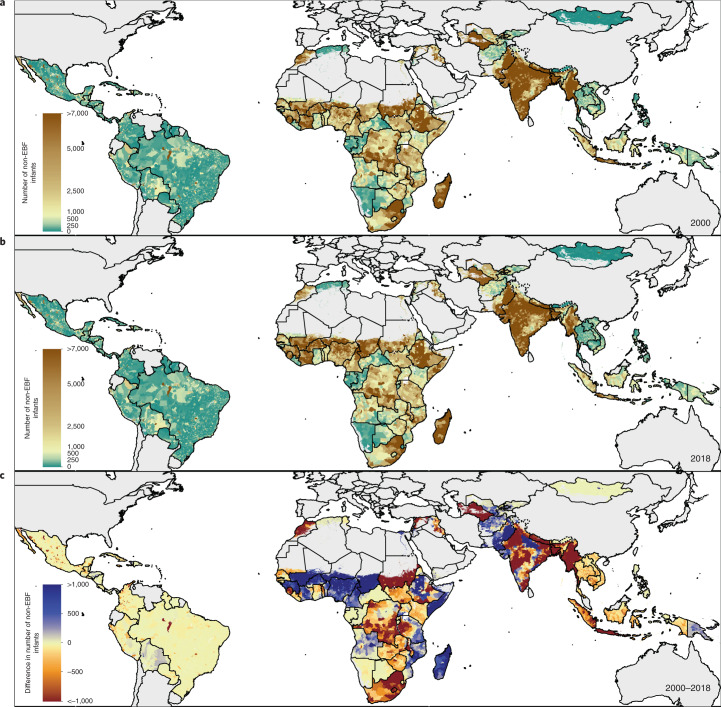
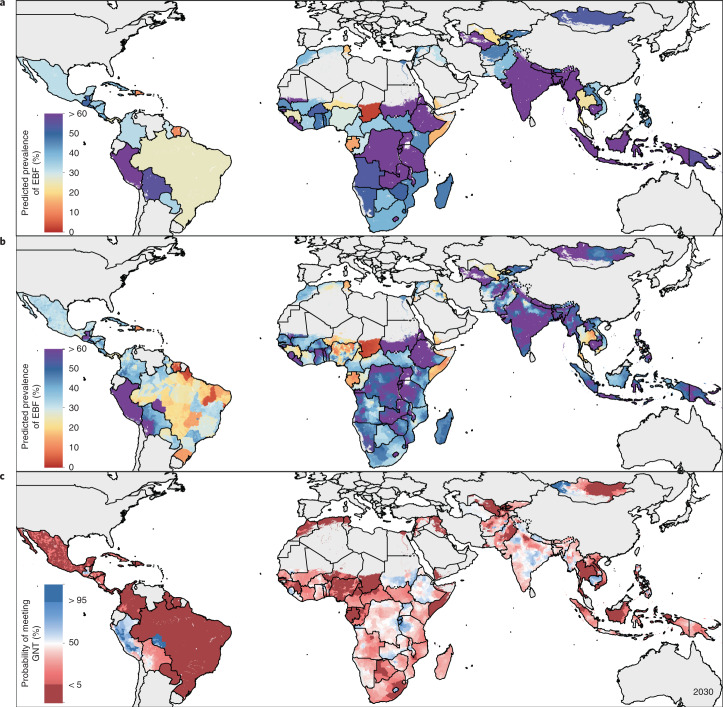
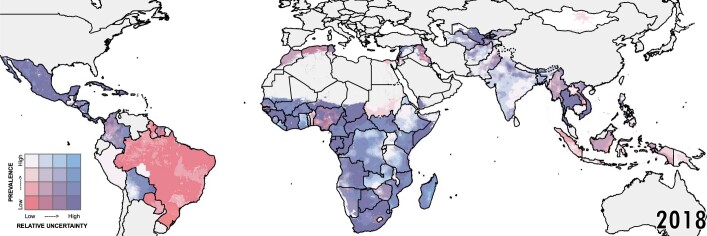
Exclusive breastfeeding (EBF)-giving infants only breast-milk for the first 6 months of life-is a component of optimal breastfeeding practices effective in preventing child morbidity and mortality. EBF practices are known to vary by population and comparable subnational estimates of prevalence and progress across low- and middle-income countries (LMICs) are required for planning policy and interventions. Here we present a geospatial analysis of EBF prevalence estimates from 2000 to 2018 across 94 LMICs mapped to policy-relevant administrative units (for example, districts), quantify subnational inequalities and their changes over time, and estimate probabilities of meeting the World Health Organization's Global Nutrition Target (WHO GNT) of ≥70% EBF prevalence by 2030. While six LMICs are projected to meet the WHO GNT of ≥70% EBF prevalence at a national scale, only three are predicted to meet the target in all their district-level units by 2030.
© 2021. The Author(s).
Conflict of interest statement
R.A. reports he received consultancy or speakers fees from UCB, Sandoz, Abbvie, Zentiva, Teva, Laropharm, CEGEDIM, Angelini, Biessen Pharma, Hofigal, AstraZeneca and Stada. A.Deshpande reports grants from Bill & Mellinda Gates Foundation, during the conduct of the study. J.J.J. reports personal fees from Boehringer Ingelheim, Zentiva, Amgen and Teva, all outside the submitted work. K.Krishan reports grants from DST PURSE and UGC Centre of Advanced Study, CAS II, awarded to the Department of Anthropology, Panjab University, Chandigarh, India, outside the submitted work. J.F.M. reports grants from Bill & Melinda Gates Foundation during the conduct of the study. S.R.P. reports non-financial support from Somnogen Canada Inc. and personal fees from editorial services, during the conduct of the study. E.U. reports having a Patent A system and method of reusable filters for anti-pollution mask pending and a Patent A system and method for electricity generation through crop stubble by using microbial fuel cells pending. All other authors declare no competing interests.
Figures
References
-
- Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: The Integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD) (WHO & UNICEF, 2013); https://www.who.int/maternal_child_adolescent/documents/global_action_pl... - PubMed
