

Segmental branches emanating from saphenous nerve morphing into sympathetic trunks for innervation of saphenous artery and its clinical implication for arterial sympathectomy
- PMID: 34085754
- PMCID: PMC8762570
- DOI: 10.1111/iwj.13630
Segmental branches emanating from saphenous nerve morphing into sympathetic trunks for innervation of saphenous artery and its clinical implication for arterial sympathectomy
Abstract
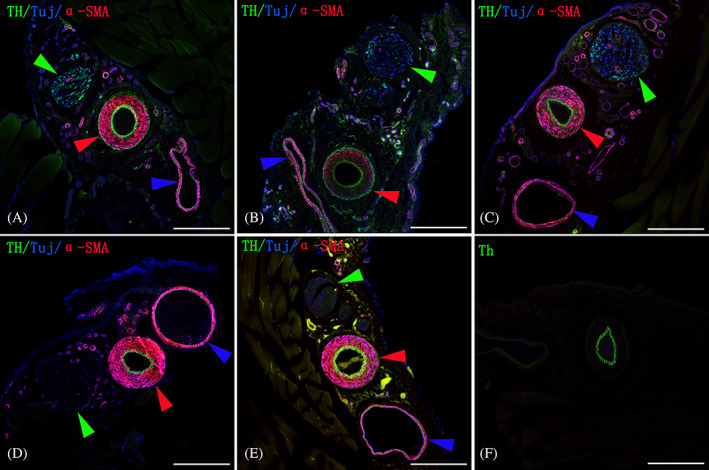
Sympathectomy of arteries has been adopted for the treatment of peripheral arterial disease and Raynaud's disease. However, the exact route for sympathetic axons to reach peripheral arteries awaits further investigation that could pave the way for development of new surgical strategies. In this study, saphenous neurovascular bundles from 10 neonatal Sprague-Dawley rats first were harvested for whole-mount immunostaining to show sympathetic innervation pattern of the artery. Secondly, 40 Sprague-Dawley male rats weighing 350 to 400 g were assigned to five groups, receiving either sham, perivascular sympathectomy, nerve-artery separation, nerve transection in the saphenous neurovascular bundle, or lumbar sympathectomy surgery that removes the lumbar sympathetic trunks. Immediately after surgery, the arterial perfusion and diameter were measured using laser speckling contrast imaging, and 1 week later the saphenous neurovascular bundles were harvested for immunostaining using antibodies against TH, neuron-specific β-tubulin (Tuj 1), and α-SMA to show the presence or absence of the TH-immuopositive staining in the adventitia. The differences among the five groups were determined using one-way analysis of variance (ANOVA). We found that an average of 2.8 ± 0.8 branches with a diameter of 4.8 ± 1.2 μm derived from the saphenous nerve that morphed into a primary and a secondary sympathetic trunk for innervation of the saphenous artery. Nerve-artery separation, nerve transection, and lumbar sympathectomy could eradicate TH-immunopositive staining of the artery, resulting, respectively, in a 12%, 36%, and 59% increase in diameter (P < .05), and a 52%, 63%, and 201% increase in perfusion compared with sham surgery (P < .01). In contrast, perivascular sympathectomy did not have a significant impact on the TH-immunopositive staining, the diameter, and perfusion of the distal part of the artery (P > .05). We conclude that the sympathetic innervation of an artery derives from segmental branches given off from its accompanying nerve. Nerve-artery disconnection is a theoretic option in sympathectomy of an artery.
Keywords: Raynaud's disease; arterial innervation; peripheral arterial disease; sympathectomy; sympathetic nerve.
© 2021 The Authors. International Wound Journal published by Medicalhelplines.com Inc (3M) and John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures






References
-
- Murata K, Omokawa S, Kobata Y, Tanaka Y, Yajima H, Tamai S. Long‐term follow‐up of periarterial sympathectomy for chronic digital ischaemia. J Hand Surg Eur Vol. 2012;37:788‐793. - PubMed
-
- Kullo IJ, Rooke TW. Clinical practice. Peripheral artery disease. N Engl J Med. 2016;374:861‐871. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter‐society consensus for the management of peripheral arterial disease (tasc ii). Eur J Vasc Endovasc Surg: Off J Eur Soc Vasc Surg. 2007;33(Suppl 1):S1‐S75. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
