

Convalescent plasma use in the USA was inversely correlated with COVID-19 mortality
- PMID: 34085928
- PMCID: PMC8205484
- DOI: 10.7554/eLife.69866
Convalescent plasma use in the USA was inversely correlated with COVID-19 mortality
Abstract
Background: The US Food and Drug Administration authorized COVID-19 convalescent plasma (CCP) therapy for hospitalized COVID-19 patients via the Expanded Access Program (EAP) and the Emergency Use Authorization (EUA), leading to use in about 500,000 patients during the first year of the pandemic for the USA.
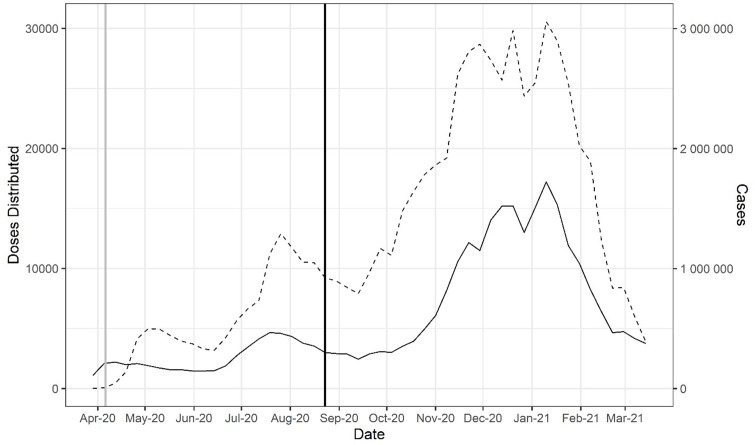
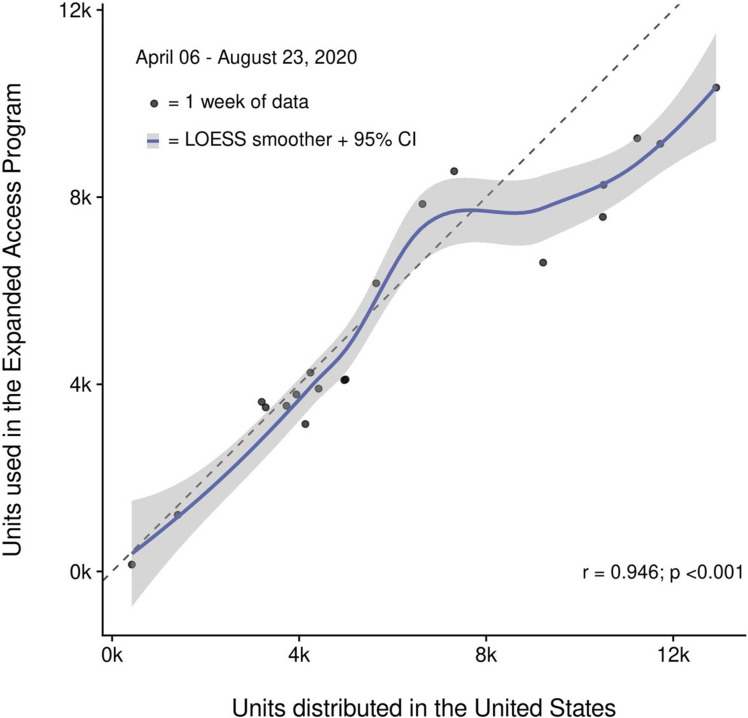
Methods: We tracked the number of CCP units dispensed to hospitals by blood banking organizations and correlated that usage with hospital admission and mortality data.
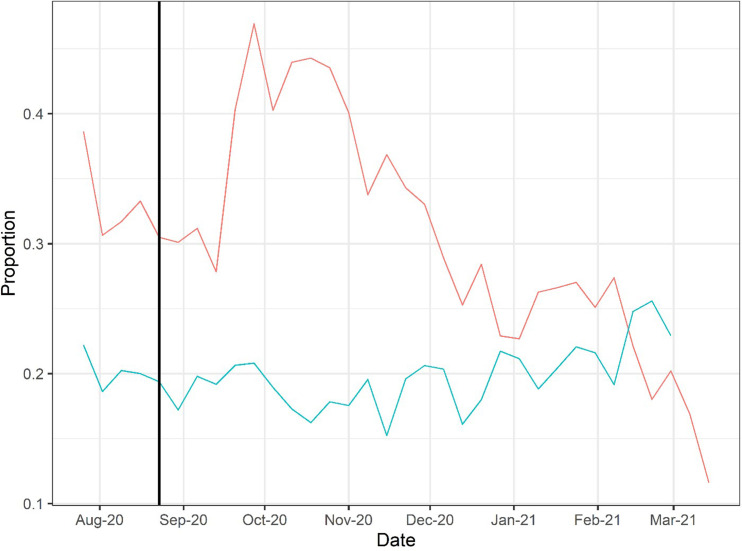
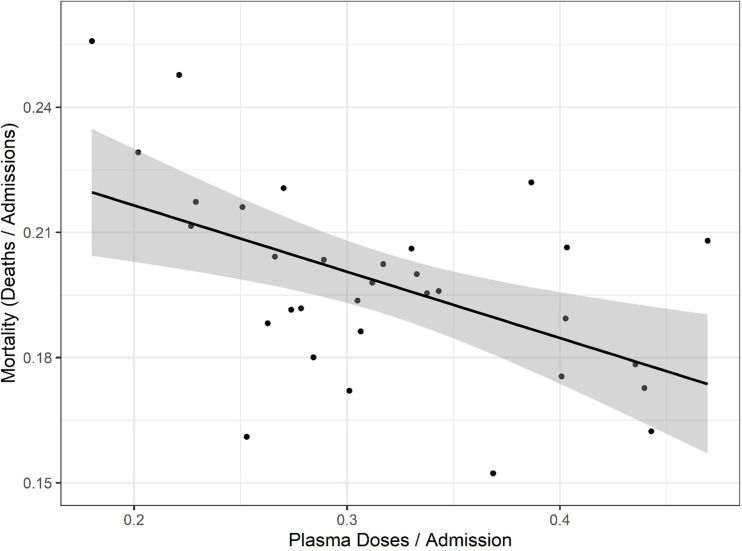
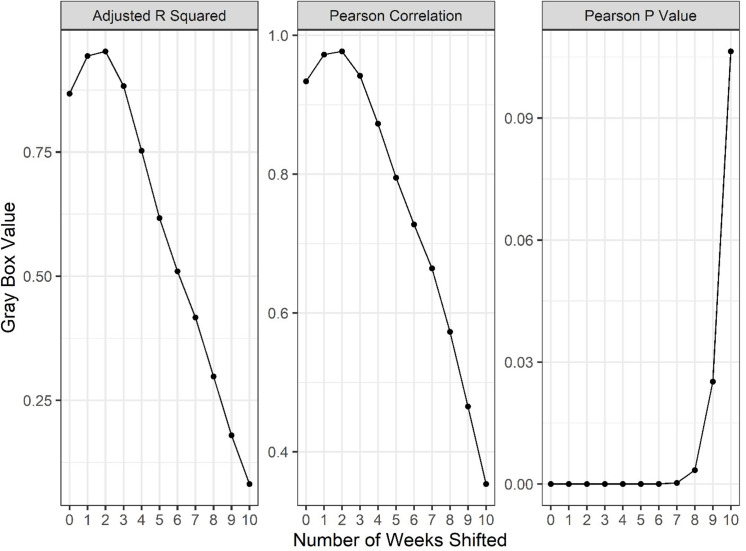
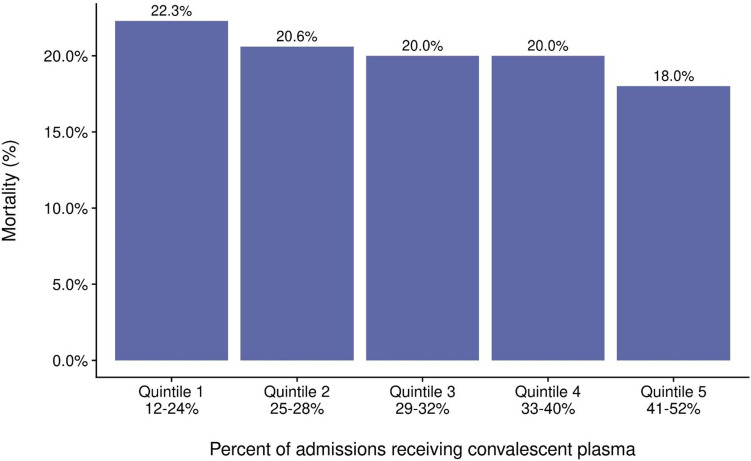
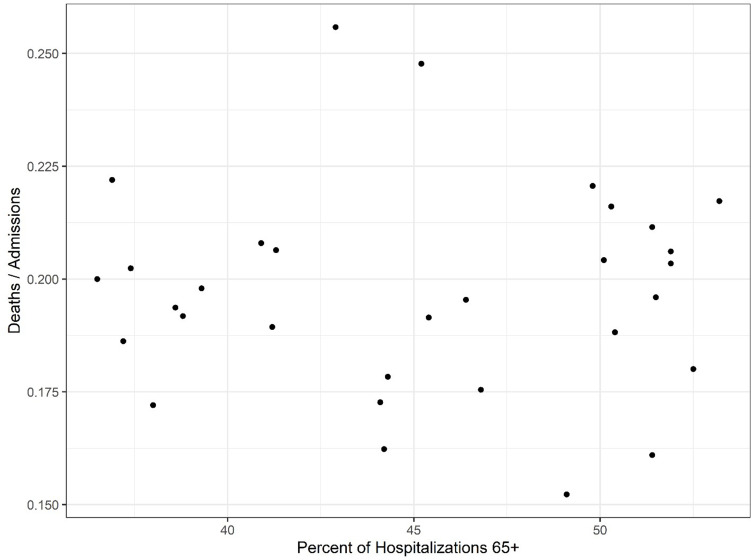
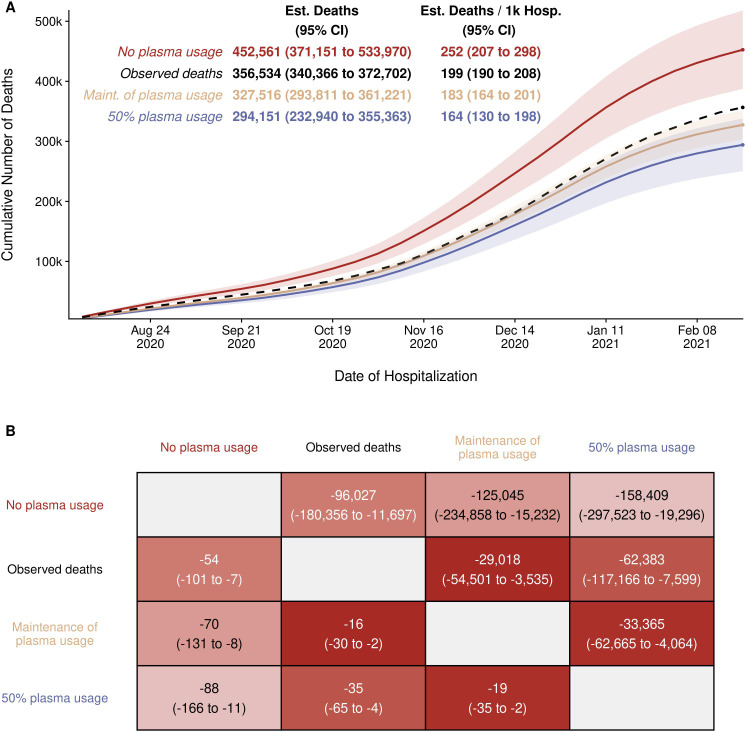
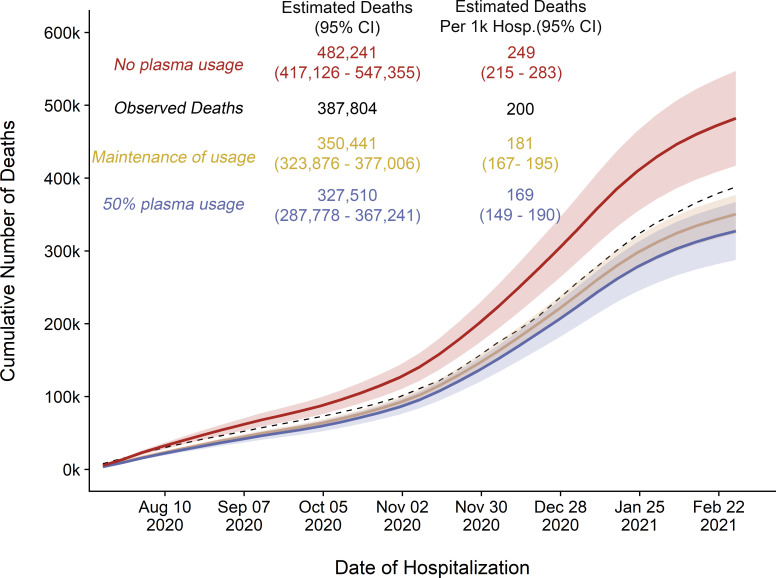
Results: CCP usage per admission peaked in Fall 2020, with more than 40% of inpatients estimated to have received CCP between late September and early November 2020. However, after randomized controlled trials failed to show a reduction in mortality, CCP usage per admission declined steadily to a nadir of less than 10% in March 2021. We found a strong inverse correlation (r = -0.52, p=0.002) between CCP usage per hospital admission and deaths occurring 2 weeks after admission, and this finding was robust to examination of deaths taking place 1, 2, or 3 weeks after admission. Changes in the number of hospital admissions, SARS-CoV-2 variants, and age of patients could not explain these findings. The retreat from CCP usage might have resulted in as many as 29,000 excess deaths from mid-November 2020 to February 2021.
Conclusions: A strong inverse correlation between CCP use and mortality per admission in the USA provides population-level evidence consistent with the notion that CCP reduces mortality in COVID-19 and suggests that the recent decline in usage could have resulted in excess deaths.
Funding: There was no specific funding for this study. AC was supported in part by RO1 HL059842 and R01 AI1520789; MJJ was supported in part by 5R35HL139854. This project has been funded in whole or in part with Federal funds from the Department of Health and Human Services; Office of the Assistant Secretary for Preparedness and Response; Biomedical Advanced Research and Development Authority under Contract No. 75A50120C00096.
Keywords: COVID; convalescent plasma; epidemiology; global health; human; virus infection.
© 2021, Casadevall et al.
Conflict of interest statement
AC, QD, PJ, JS, SK, RW, MJ, NP, RC No competing interests declared
Figures
Update of
-
Convalescent Plasma Use in the United States was inversely correlated with COVID-19 Mortality: Did Plasma Hesitancy cost lives?medRxiv [Preprint]. 2021 Apr 16:2021.04.07.21255089. doi: 10.1101/2021.04.07.21255089. medRxiv. 2021. Update in: Elife. 2021 Jun 04;10:e69866. doi: 10.7554/eLife.69866. PMID: 33851186 Free PMC article. Updated. Preprint.
References
-
- Acosta-Ampudia Y, Monsalve DM, Rojas M, Rodríguez Y, Gallo JE, Salazar-Uribe JC, Santander MJ, Cala MP, Zapata W, Zapata MI, Manrique R, Pardo-Oviedo JM, Camacho B, Ramírez-Santana C, Anaya JM, CP-COVID-19 group COVID-19 convalescent plasma composition and immunological effects in severe patients. Journal of Autoimmunity. 2021;118:102598. doi: 10.1016/j.jaut.2021.102598. - DOI - PMC - PubMed
-
- Agarwal A, Mukherjee A, Kumar G, Chatterjee P, Bhatnagar T, Malhotra P, PLACID Trial Collaborators Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID trial) BMJ. 2020;371:m3939. doi: 10.1136/bmj.m3939. - DOI - PMC - PubMed
-
- Anonymous AABB survey: ccp usage reevaluation march. 2021a. [April 1, 2021]. https://www.aabb.org/docs/default-source/default-document-library/resour...
-
- Anonymous Investigational COVID-19 convalescent plasma, Guidance for Industry. 2021b. [April 1, 2021]. https://www.fda.gov/regulatory-information/search-fda-guidance-documents...
-
- Anonymous Variant proportions in the united states. 2021c. [April 1, 2021]. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-proporti...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
