

Living donor liver transplantation for Budd‒Chiari syndrome with right posterior segment graft and patch plasty using the superficial femoral vein: a case report
- PMID: 34086114
- PMCID: PMC8178427
- DOI: 10.1186/s40792-021-01224-5
Living donor liver transplantation for Budd‒Chiari syndrome with right posterior segment graft and patch plasty using the superficial femoral vein: a case report
Abstract
Background: In living donor liver transplantation (LDLT) for patients with Budd‒Chiari syndrome (BCS), there are several concerns about reconstruction of the inferior vena cava (IVC) and hepatic veins. Herein, we report the case of a patient with BCS who underwent LDLT with right posterior segment graft (RPSG) and patch plasty for reconstruction of the hepatic venous outflow, using the patient's own superficial femoral vein (SFV).
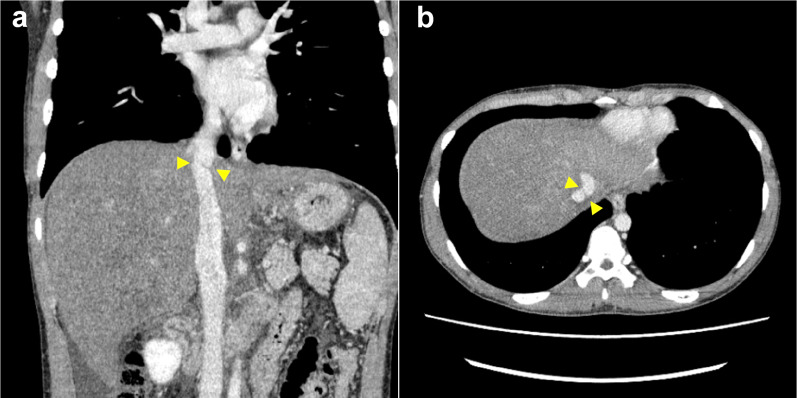
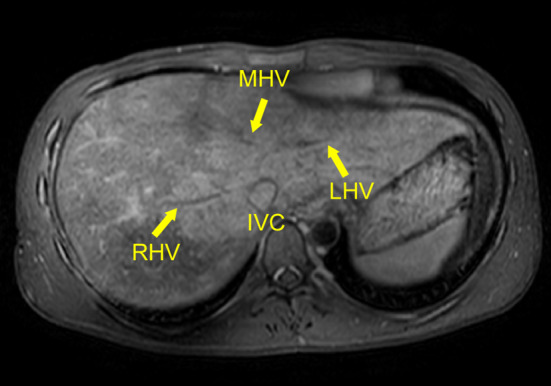
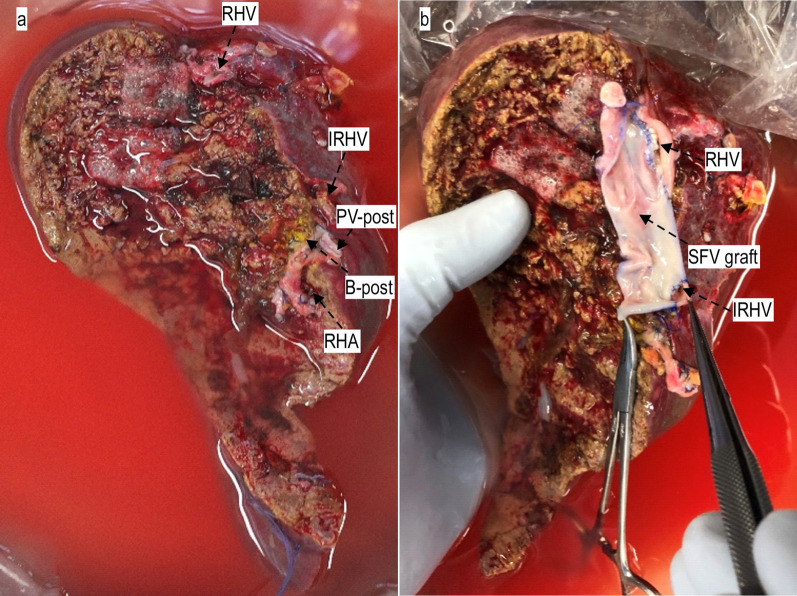
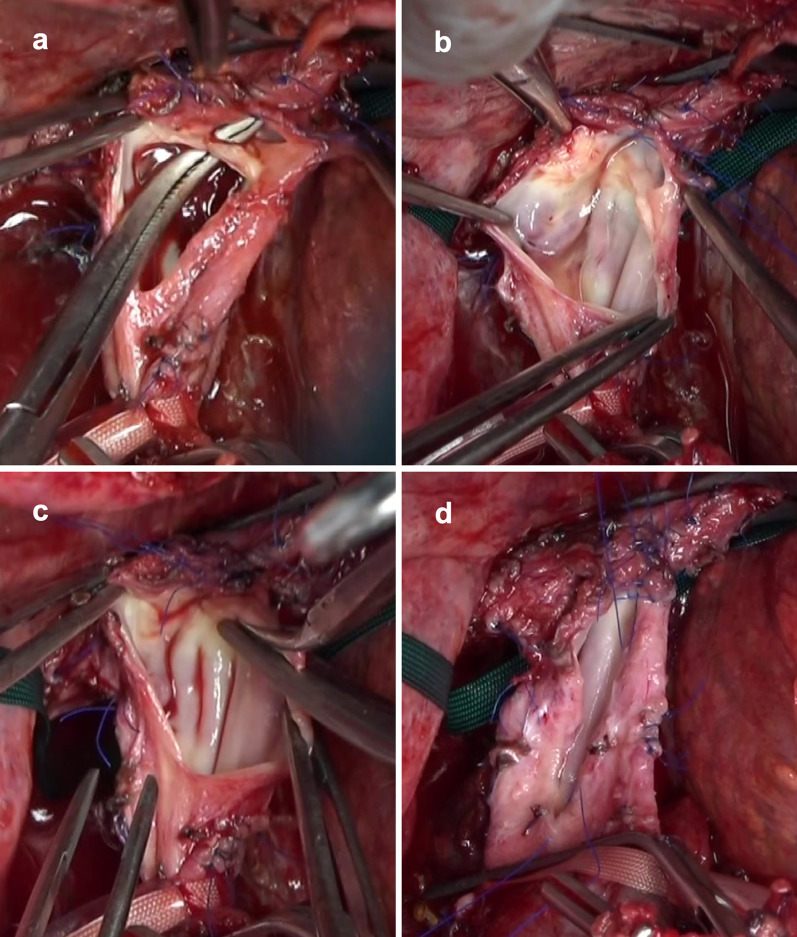
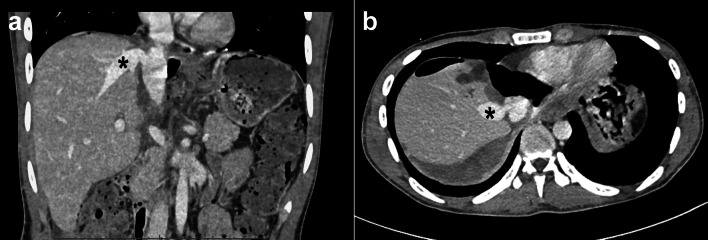
Case presentation: A 19-year-old man, who was diagnosed with primary BCS, underwent LDLT. His main hepatic veins were totally obstructed, and membranous stenosis was seen in the IVC. The LDLT donor was his mother; however, liver volumetric analysis showed that only her RPSG was appropriate. In the recipient surgery, 16 cm of the left SFV was harvested and was cut longitudinally and opened. The right hepatic vein (RHV) of the RPSG was anastomosed to the sidewall of the SFV graft. After explantation of native diseased liver was completed, the stenotic and thickened wall of the IVC was widely resected, and a large anastomotic orifice was created. Patch cavoplasty was performed with the RHV‒SFV graft patch. After portal reperfusion started, hepatic venous outflow was satisfactory, and there was no venous graft congestion. Both his postoperative course and his long-term course after discharge were uneventful.
Conclusions: In LDLT for BCS patients, ingenuity is required for the reconstruction of venous outflow. The SFV patch can be safely harvested from liver transplant recipients and is suitable for venous reconstruction. In addition, RPSG is an alternative type of liver graft for LDLT if a conventional right- or left-lobe graft cannot be used.
Keywords: Budd‒Chiari syndrome; Living donor liver transplantation; Right posterior segment graft; Superficial femoral vein.
Conflict of interest statement
The authors declare that they have no conflicts of interests.
Figures
Similar articles
-
Hepatic venous reconstruction using the superficial femoral vein in a right-lobe living donor liver transplant patient with interrupted inferior vena cava.Pediatr Transplant. 2014 Feb;18(1):E13-7. doi: 10.1111/petr.12191. Epub 2013 Nov 25. Pediatr Transplant. 2014. PMID: 24384053
-
Immunohistochemical evaluation for outflow reconstruction using opened round ligament in living donor right posterior sector graft liver transplantation: A case report.World J Gastroenterol. 2016 Sep 14;22(34):7851-6. doi: 10.3748/wjg.v22.i34.7851. World J Gastroenterol. 2016. PMID: 27678368 Free PMC article.
-
New Left Lobe Transplantation Procedure with Caval Reconstruction Using an Inverted Composite Graft for Chronic Budd-Chiari Syndrome in Living-Donor Liver Transplantation-A Case Report.Transplant Proc. 2018 May;50(4):1192-1195. doi: 10.1016/j.transproceed.2017.11.078. Transplant Proc. 2018. PMID: 29731092
-
Living donor liver transplantation for idiopathic portal hypertension with extrahepatic portal vein stenosis and splenic artery aneurysms: a case report and review of the literature.BMC Surg. 2020 Oct 29;20(1):257. doi: 10.1186/s12893-020-00921-6. BMC Surg. 2020. PMID: 33121468 Free PMC article. Review.
-
Standardized surgical techniques for adult living donor liver transplantation using a modified right lobe graft: a video presentation from bench to reperfusion.Korean J Hepatobiliary Pancreat Surg. 2016 Aug;20(3):97-101. doi: 10.14701/kjhbps.2016.20.3.97. Epub 2016 Aug 29. Korean J Hepatobiliary Pancreat Surg. 2016. PMID: 27621745 Free PMC article. Review.
References
-
- Sugawara Y, Makuuchi M, Takayama T, Mizuta K, Kawarasaki H, Imamura H, et al. Liver transplantation using a right lateral sector graft from a living donor to her granddaughter. Hepatogastroenterology. 2001;48:261–263. - PubMed
-
- Valla DC. Hepatic venous outflow tract obstruction etiopathogenesis: Asia versus the West. J Gastroenterol Hepatol. 2004;19:S204–S211. doi: 10.1111/j.1440-1746.2004.03642.x. - DOI
LinkOut - more resources
Full Text Sources
