

Oxygen Toxicity in Critically Ill Adults
- PMID: 34086536
- PMCID: PMC8521700
- DOI: 10.1164/rccm.202102-0417CI
Oxygen Toxicity in Critically Ill Adults
Abstract
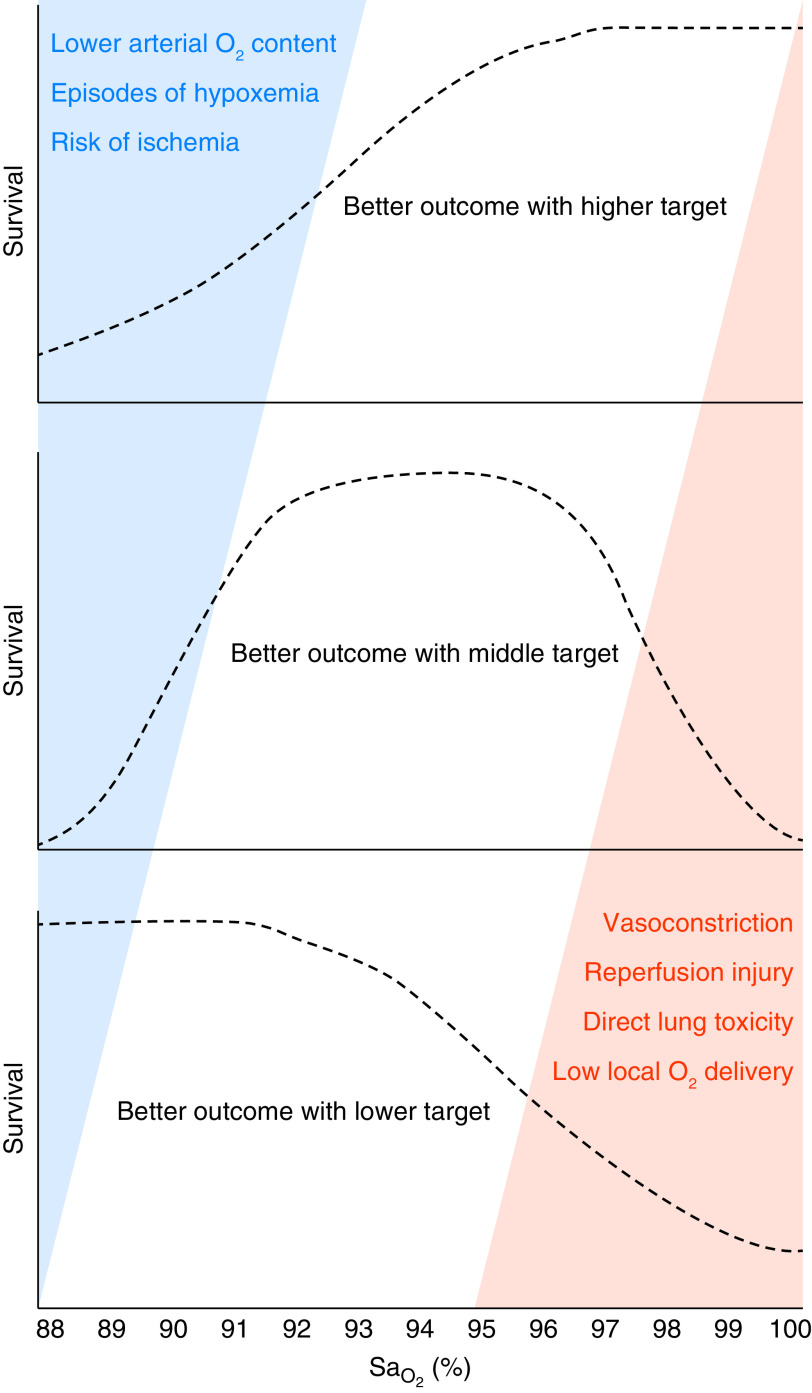
Oxygen supplementation is one of the most common interventions in critically ill patients. Despite over a century of data suggesting both beneficial and detrimental effects of supplemental oxygen, optimal arterial oxygenation targets in adult patients remain unclear. Laboratory animal studies have consistently showed that exposure to a high FiO2 causes respiratory failure and early death. Human autopsy studies from the 1960s purported to provide histologic evidence of pulmonary oxygen toxicity in the form of diffuse alveolar damage. However, concomitant ventilator-induced lung injury and/or other causes of acute lung injury may explain these findings. Although some observational studies in general populations of critically adults showed higher mortality in association with higher oxygen exposures, this finding has not been consistent. For some specific populations, such as those with cardiac arrest, studies have suggested harm from targeting supraphysiologic PaO2 levels. More recently, randomized clinical trials of arterial oxygenation targets in narrower physiologic ranges were conducted in critically ill adult patients. Although two smaller trials came to opposite conclusions, the two largest of these trials showed no differences in clinical outcomes in study groups that received conservative versus liberal oxygen targets, suggesting that either strategy is reasonable. It is possible that some strategies are of benefit in some subpopulations, and this remains an important ongoing area of research. Because of the ubiquity of oxygen supplementation in critically ill adults, even small treatment effects could have a large impact on a global scale.
Keywords: ICUs; hyperoxia; oxygen inhalational therapy.
Figures
References
-
- West JB. Joseph Priestley, oxygen, and the enlightenment. Am J Physiol Lung Cell Mol Physiol. 2014;306:L111–L119. - PubMed
-
- Warren CPW. The introduction of oxygen for pneumonia as seen through the writings of two McGill University professors, William Osler and Jonathan Meakins. Can Respir J. 2005;12:81–85. - PubMed
-
- Clark JM, Lambertsen CJ. Pulmonary oxygen toxicity: a review. Pharmacol Rev. 1971;23:37–133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
