

Ambulatory Risk Models for the Long-Term Prevention of Sepsis: Retrospective Study
- PMID: 34086596
- PMCID: PMC8299345
- DOI: 10.2196/29986
Ambulatory Risk Models for the Long-Term Prevention of Sepsis: Retrospective Study
Abstract
Background: Sepsis is a life-threatening condition that can rapidly lead to organ damage and death. Existing risk scores predict outcomes for patients who have already become acutely ill.
Objective: We aimed to develop a model for identifying patients at risk of getting sepsis within 2 years in order to support the reduction of sepsis morbidity and mortality.
Methods: Machine learning was applied to 2,683,049 electronic health records (EHRs) with over 64 million encounters across five states to develop models for predicting a patient's risk of getting sepsis within 2 years. Features were selected to be easily obtainable from a patient's chart in real time during ambulatory encounters.
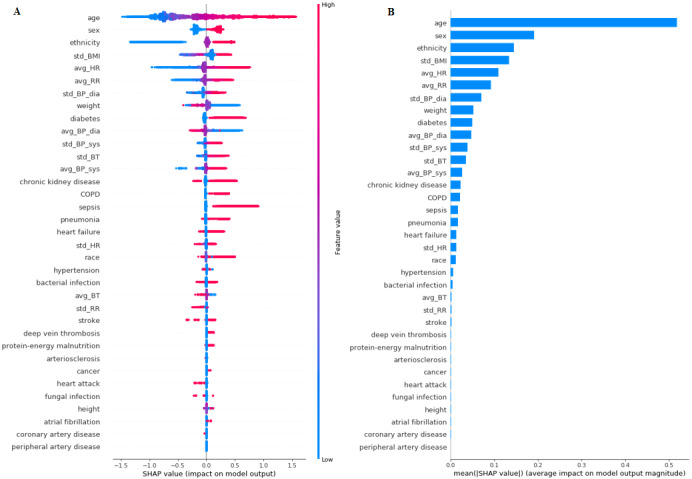
Results: The models showed consistent prediction scores, with the highest area under the receiver operating characteristic curve of 0.82 and a positive likelihood ratio of 2.9 achieved with gradient boosting on all features combined. Predictive features included age, sex, ethnicity, average ambulatory heart rate, standard deviation of BMI, and the number of prior medical conditions and procedures. The findings identified both known and potential new risk factors for long-term sepsis. Model variations also illustrated trade-offs between incrementally higher accuracy, implementability, and interpretability.
Conclusions: Accurate implementable models were developed to predict the 2-year risk of sepsis, using EHR data that is easy to obtain from ambulatory encounters. These results help advance the understanding of sepsis and provide a foundation for future trials of risk-informed preventive care.
Keywords: clinical decision making; electronic health records; machine learning; prevention; risk factors; risk prediction; sepsis.
©Jewel Y Lee, Sevda Molani, Chen Fang, Kathleen Jade, D Shane O'Mahony, Sergey A Kornilov, Lindsay T Mico, Jennifer J Hadlock. Originally published in JMIR Medical Informatics (https://medinform.jmir.org), 08.07.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures





Similar articles
-
Prediction of In-hospital Mortality in Emergency Department Patients With Sepsis: A Local Big Data-Driven, Machine Learning Approach.Acad Emerg Med. 2016 Mar;23(3):269-78. doi: 10.1111/acem.12876. Epub 2016 Feb 13. Acad Emerg Med. 2016. PMID: 26679719 Free PMC article.
-
Using machine learning methods to predict in-hospital mortality of sepsis patients in the ICU.BMC Med Inform Decis Mak. 2020 Oct 2;20(1):251. doi: 10.1186/s12911-020-01271-2. BMC Med Inform Decis Mak. 2020. PMID: 33008381 Free PMC article.
-
Tensor learning of pointwise mutual information from EHR data for early prediction of sepsis.Comput Biol Med. 2021 Jul;134:104430. doi: 10.1016/j.compbiomed.2021.104430. Epub 2021 May 7. Comput Biol Med. 2021. PMID: 33991856
-
Utilizing time series data embedded in electronic health records to develop continuous mortality risk prediction models using hidden Markov models: A sepsis case study.Stat Methods Med Res. 2020 Nov;29(11):3409-3423. doi: 10.1177/0962280220929045. Epub 2020 Jun 17. Stat Methods Med Res. 2020. PMID: 32552573
-
A Machine-Learning Approach for Dynamic Prediction of Sepsis-Induced Coagulopathy in Critically Ill Patients With Sepsis.Front Med (Lausanne). 2021 Jan 21;7:637434. doi: 10.3389/fmed.2020.637434. eCollection 2020. Front Med (Lausanne). 2021. PMID: 33553224 Free PMC article.
Cited by
-
Risk factors for severe COVID-19 differ by age for hospitalized adults.Sci Rep. 2022 Apr 28;12(1):6568. doi: 10.1038/s41598-022-10344-3. Sci Rep. 2022. PMID: 35484176 Free PMC article.
References
-
- Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, Kadri SS, Angus DC, Danner RL, Fiore AE, Jernigan JA, Martin GS, Septimus E, Warren DK, Karcz A, Chan C, Menchaca JT, Wang R, Gruber S, Klompas M, CDC Prevention Epicenter Program Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014. JAMA. 2017 Oct 03;318(13):1241–1249. doi: 10.1001/jama.2017.13836. http://europepmc.org/abstract/MED/28903154 - DOI - PMC - PubMed
-
- Novosad SA, Sapiano MR, Grigg C, Lake J, Robyn M, Dumyati G, Felsen C, Blog D, Dufort E, Zansky S, Wiedeman K, Avery L, Dantes RB, Jernigan JA, Magill SS, Fiore A, Epstein L. Vital Signs: Epidemiology of Sepsis: Prevalence of Health Care Factors and Opportunities for Prevention. MMWR Morb Mortal Wkly Rep. 2016 Aug 26;65(33):864–9. doi: 10.15585/mmwr.mm6533e1. doi: 10.15585/mmwr.mm6533e1. - DOI - DOI - PubMed
-
- Fleischmann C, Scherag A, Adhikari NKJ, Hartog CS, Tsaganos T, Schlattmann P, Angus DC, Reinhart K, International Forum of Acute Care Trialists Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am J Respir Crit Care Med. 2016 Feb 01;193(3):259–72. doi: 10.1164/rccm.201504-0781OC. - DOI - PubMed
LinkOut - more resources
Full Text Sources
