

Plasma ACE2 predicts outcome of COVID-19 in hospitalized patients
- PMID: 34086837
- PMCID: PMC8177449
- DOI: 10.1371/journal.pone.0252799
Plasma ACE2 predicts outcome of COVID-19 in hospitalized patients
Abstract
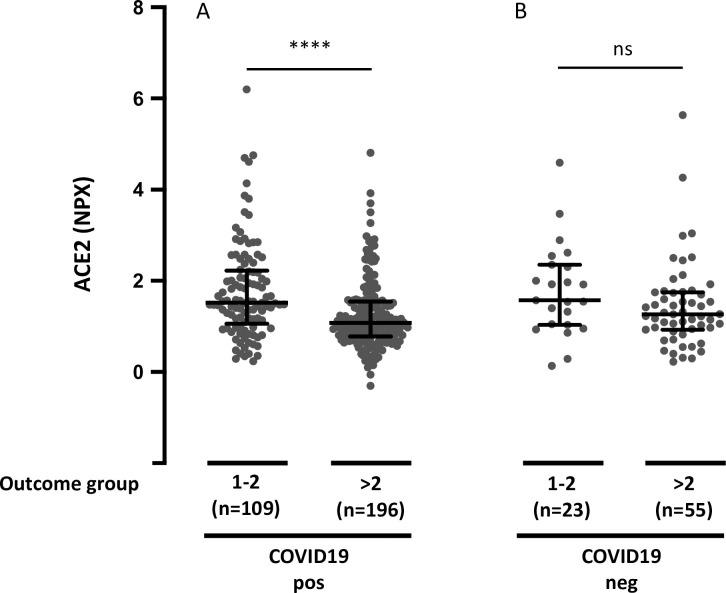
Aims: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) binds to angiotensin converting enzyme 2 (ACE2) enabling entrance of the virus into cells and causing the infection termed coronavirus disease of 2019 (COVID-19). Here, we investigate associations between plasma ACE2 and outcome of COVID-19.
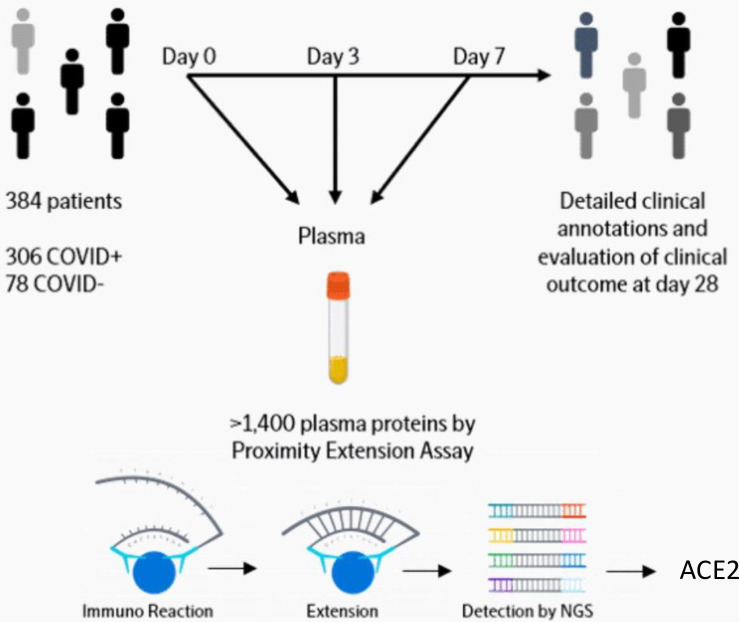
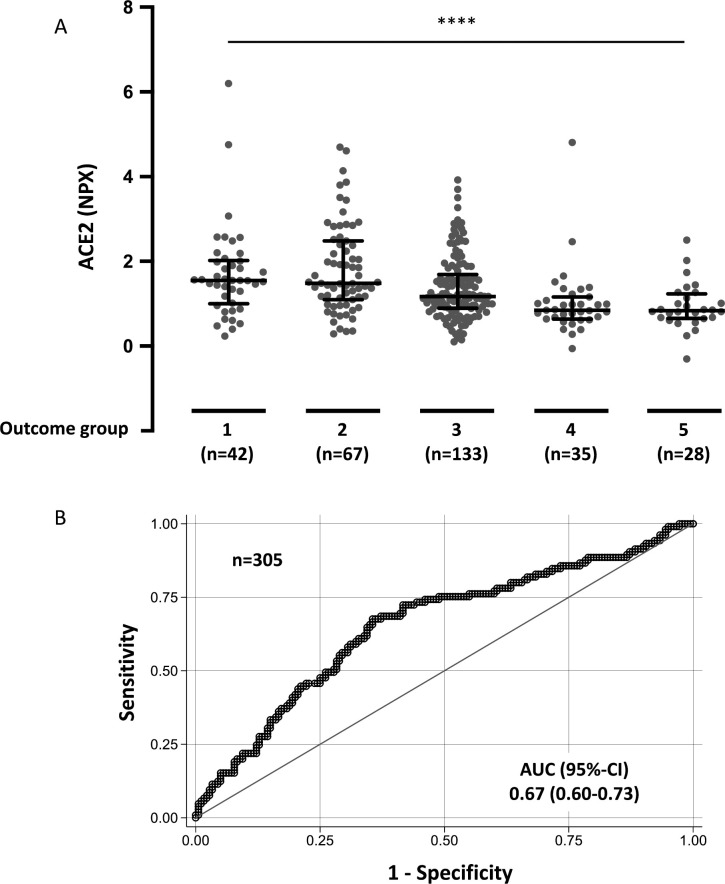
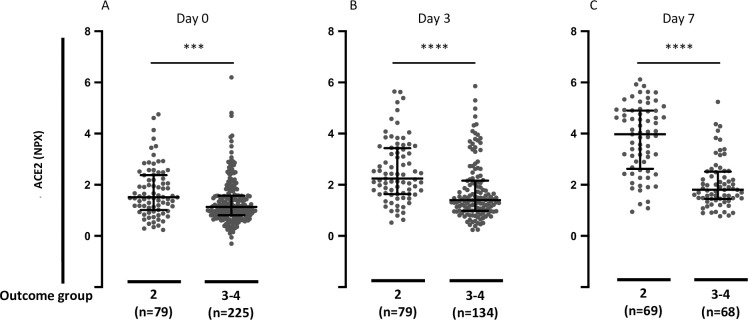
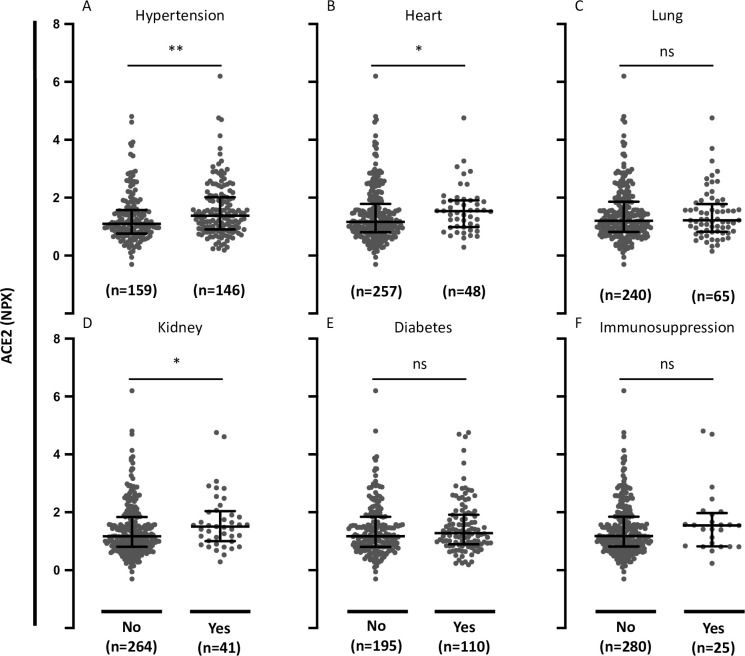
Methods and results: This analysis used data from a large longitudinal study of 306 COVID-19 positive patients and 78 COVID-19 negative patients (MGH Emergency Department COVID-19 Cohort). Comprehensive clinical data were collected on this cohort, including 28-day outcomes. The samples were run on the Olink® Explore 1536 platform which includes measurement of the ACE2 protein. High admission plasma ACE2 in COVID-19 patients was associated with increased maximal illness severity within 28 days with OR = 1.8, 95%-CI: 1.4-2.3 (P < 0.0001). Plasma ACE2 was significantly higher in COVID-19 patients with hypertension compared with patients without hypertension (P = 0.0045). Circulating ACE2 was also significantly higher in COVID-19 patients with pre-existing heart conditions and kidney disease compared with patients without these pre-existing conditions (P = 0.0363 and P = 0.0303, respectively).
Conclusion: This study suggests that measuring plasma ACE2 is potentially valuable in predicting COVID-19 outcomes. Further, ACE2 could be a link between COVID-19 illness severity and its established risk factors hypertension, pre-existing heart disease and pre-existing kidney disease.
Conflict of interest statement
IG is an employee of Olink Proteomics. This does not alter our adherence to PLOS ONE policies on sharing data and materials. The authors declare no other potential conflicts of interest.
Figures

References
-
- Banerjee A, Pasea L, Harris S, Gonzalez-Izquierdo A, Torralbo A, Shallcross L, et al.. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: a population-based cohort study. Lancet. 2020;395(10238):1715–25. doi: 10.1016/S0140-6736(20)30854-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
