

Coronary artery calcium is associated with increased risk for lung and colorectal cancer in men and women: the Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 34086883
- PMCID: PMC9016360
- DOI: 10.1093/ehjci/jeab099
Coronary artery calcium is associated with increased risk for lung and colorectal cancer in men and women: the Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Aims: This study explored the association of coronary artery calcium (CAC) with incident cancer subtypes in the Multi-Ethnic Study of Atherosclerosis (MESA). CAC is an established predictor of cardiovascular disease (CVD), with emerging data also supporting independent predictive value for cancer. The association of CAC with risk for individual cancer subtypes is unknown.
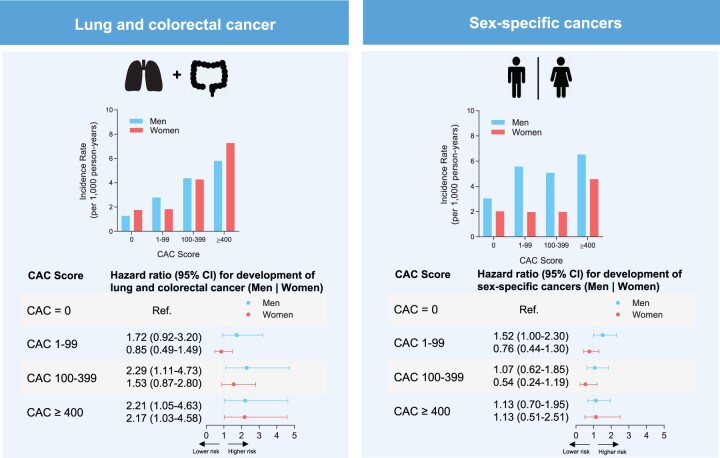
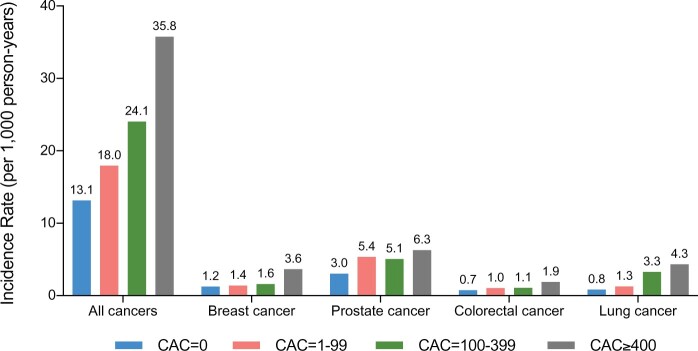
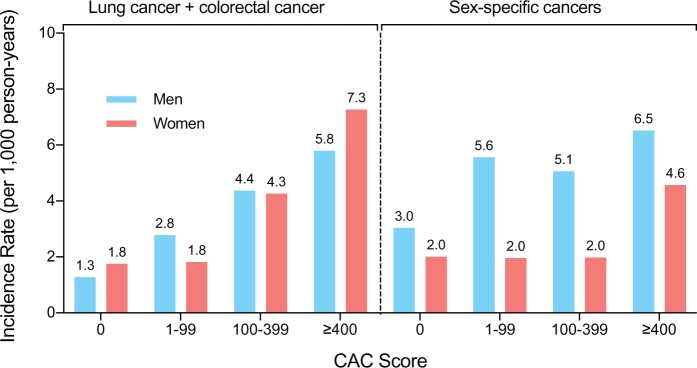
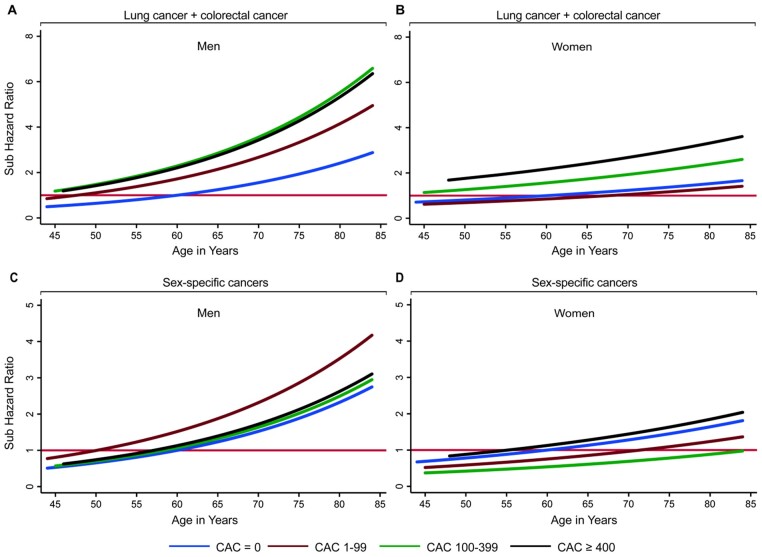
Methods and results: We included 6271 MESA participants, aged 45-84 and without known CVD or self-reported history of cancer. There were 777 incident cancer cases during mean follow-up of 12.9 ± 3.1 years. Lung and colorectal cancer (186 cases) were grouped based on their strong overlap with CVD risk profile; prostate (men) and ovarian, uterine, and breast cancer (women) were considered as sex-specific cancers (in total 250 cases). Incidence rates and Fine and Gray competing risks models were used to assess relative risk of cancer-specific outcomes stratified by CAC groups or Log(CAC+1). The mean age was 61.7 ± 10.2 years, 52.7% were women, and 36.5% were White. Overall, all-cause cancer incidence increased with CAC scores, with rates per 1000 person-years of 13.1 [95% confidence interval (CI): 11.7-14.7] for CAC = 0 and 35.8 (95% CI: 30.2-42.4) for CAC ≥400. Compared with CAC = 0, hazards for those with CAC ≥400 were increased for lung and colorectal cancer in men [subdistribution hazard ratio (SHR): 2.2 (95% CI: 1.1-4.7)] and women [SHR: 2.2 (95% CI: 1.0-4.6)], but not significantly for sex-specific cancers across sexes.
Conclusion: CAC scores were associated with cancer risk in both sexes; however, this was stronger for lung and colorectal when compared with sex-specific cancers. Our data support potential synergistic use of CAC scores in the identification of both CVD and lung and colorectal cancer risk.
Keywords: cancer; cardiovascular disease; coronary arterial calcium; prevention; risk prediction.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Blaha MJ, Silverman MG, Budoff MJ. Is there a role for coronary artery calcium scoring for management of asymptomatic patients at risk for coronary artery disease?: clinical risk scores are not sufficient to define primary prevention treatment strategies among asymptomatic patients. Circ Cardiovasc Imaging 2014;7:398–408; discussion 408. - PubMed
-
- Hecht HS. Coronary artery calcium scanning: past, present, and future. JACC Cardiovasc Imaging 2015;8:579–96. - PubMed
-
- Dzaye O, Dudum R, Mirbolouk M, Orimoloye OA, Osei AD, Dardari ZA et al. Validation of the Coronary Artery Calcium Data and Reporting System (CAC-DRS): dual importance of CAC score and CAC distribution from the Coronary Artery Calcium (CAC) consortium. J Cardiovasc Comput Tomogr 2020;14:12–7. - PMC - PubMed
-
- Blaha MJ, Cainzos-Achirica M, Dardari Z, Blankstein R, Shaw LJ, Rozanski A et al. All-cause and cause-specific mortality in individuals with zero and minimal coronary artery calcium: a long-term, competing risk analysis in the Coronary Artery Calcium Consortium. Atherosclerosis 2020;294:72–9. - PMC - PubMed
-
- Dzaye O, Dudum R, Reiter-Brennan C, Kianoush S, Tota-Maharaj R, Cainzos-Achirica M et al. Coronary artery calcium scoring for individualized cardiovascular risk estimation in important patient subpopulations after the 2019 AHA/ACC primary prevention guidelines. Prog Cardiovasc Dis 2019;62:423–30. - PubMed
MeSH terms
Substances
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- National Center for Advancing Translational Sciences (NCATS)
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- UL1-TR-000040/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
