

Influence of supramarginal resection on survival outcomes after gross-total resection of IDH-wild-type glioblastoma
- PMID: 34087795
- PMCID: PMC9248270
- DOI: 10.3171/2020.10.JNS203366
Influence of supramarginal resection on survival outcomes after gross-total resection of IDH-wild-type glioblastoma
Abstract
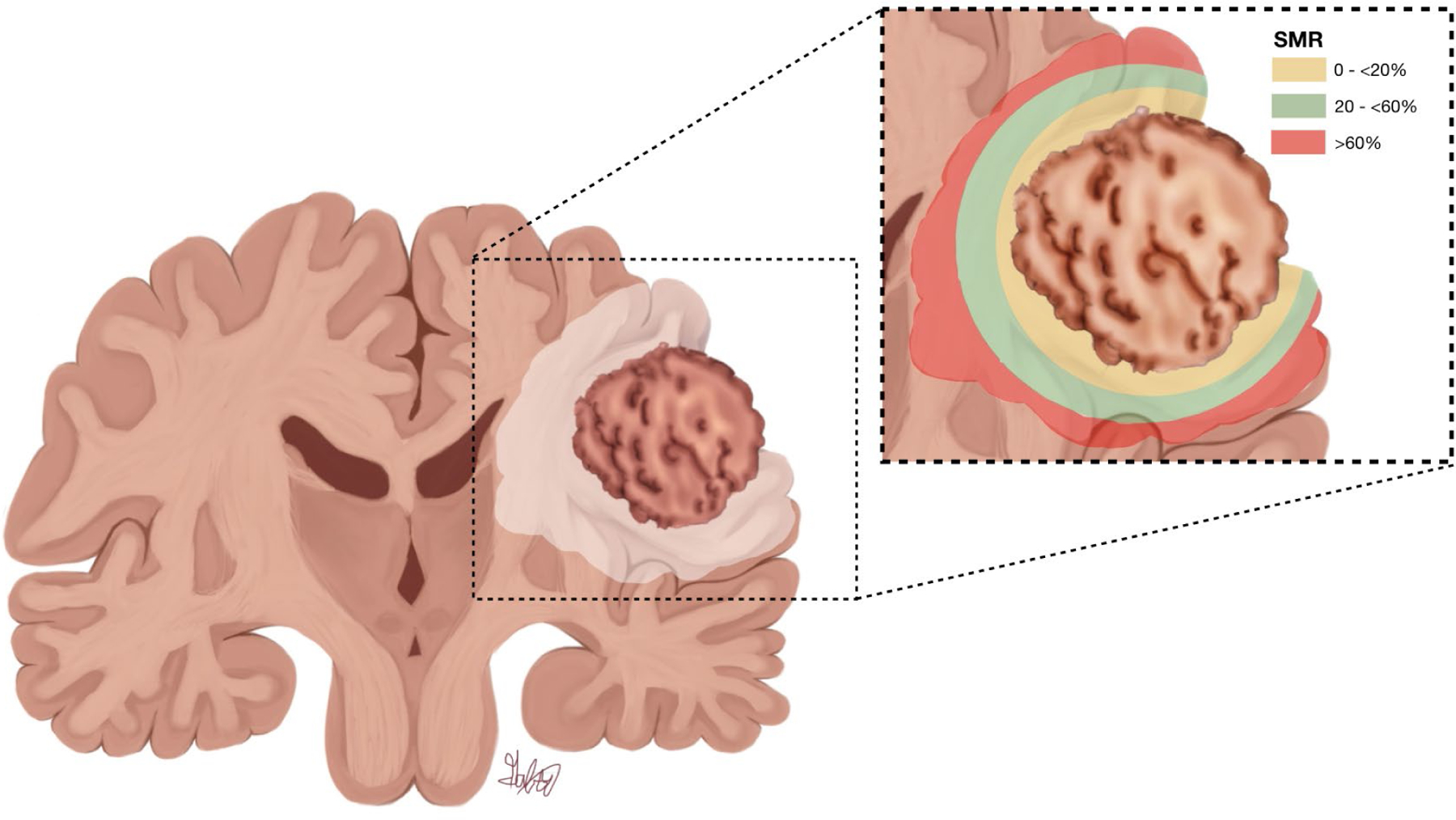
Objective: The authors' goal was to use a multicenter, observational cohort study to determine whether supramarginal resection (SMR) of FLAIR-hyperintense tumor beyond the contrast-enhanced (CE) area influences the overall survival (OS) of patients with isocitrate dehydrogenase-wild-type (IDH-wt) glioblastoma after gross-total resection (GTR).
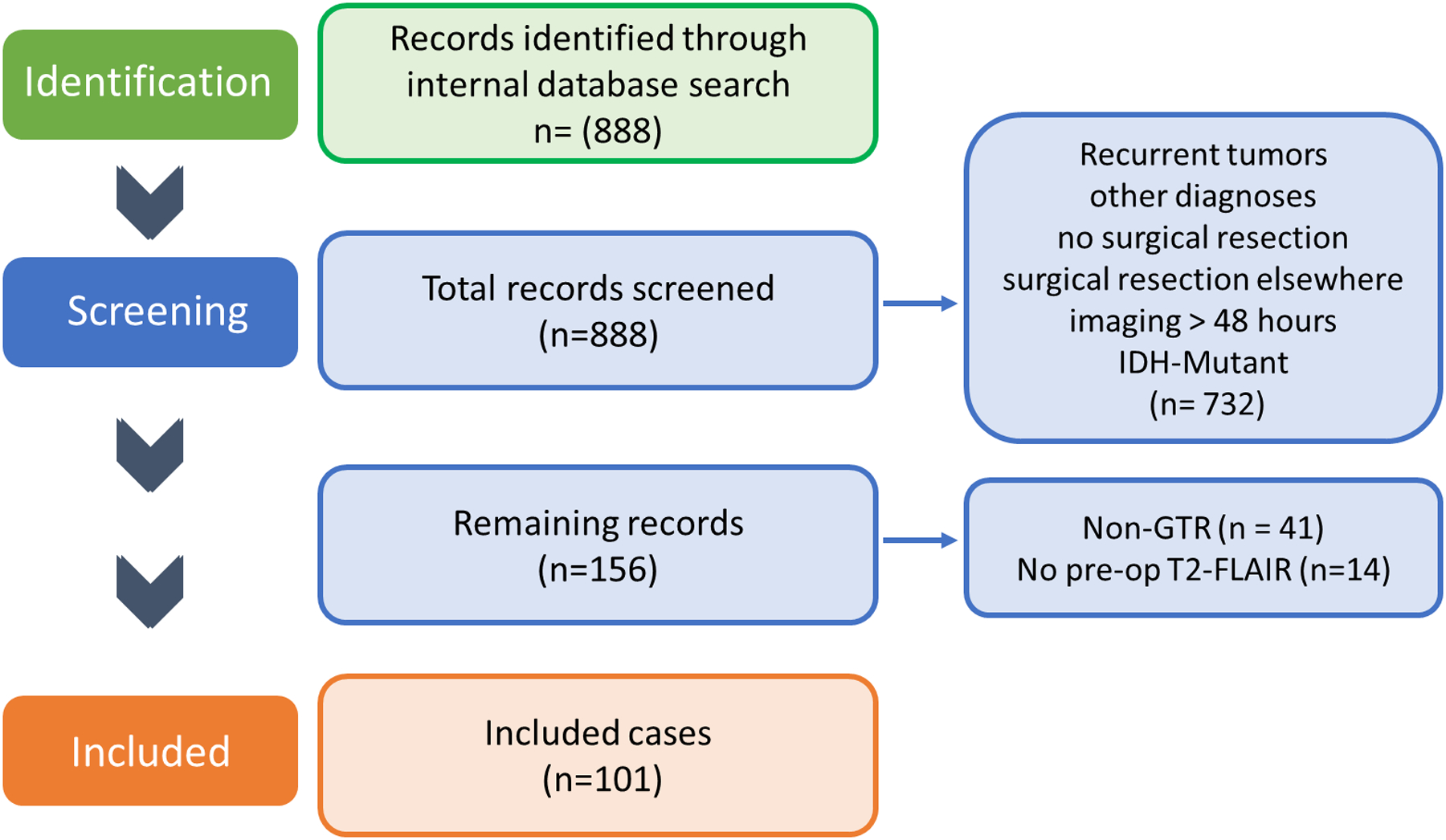
Methods: The medical records of 888 patients aged ≥ 18 years who underwent resection of GBM between January 2011 and December 2017 were reviewed. Volumetric measurements of the CE tumor and surrounding FLAIR-hyperintense tumor were performed, clinical variables were obtained, and associations with OS were analyzed.
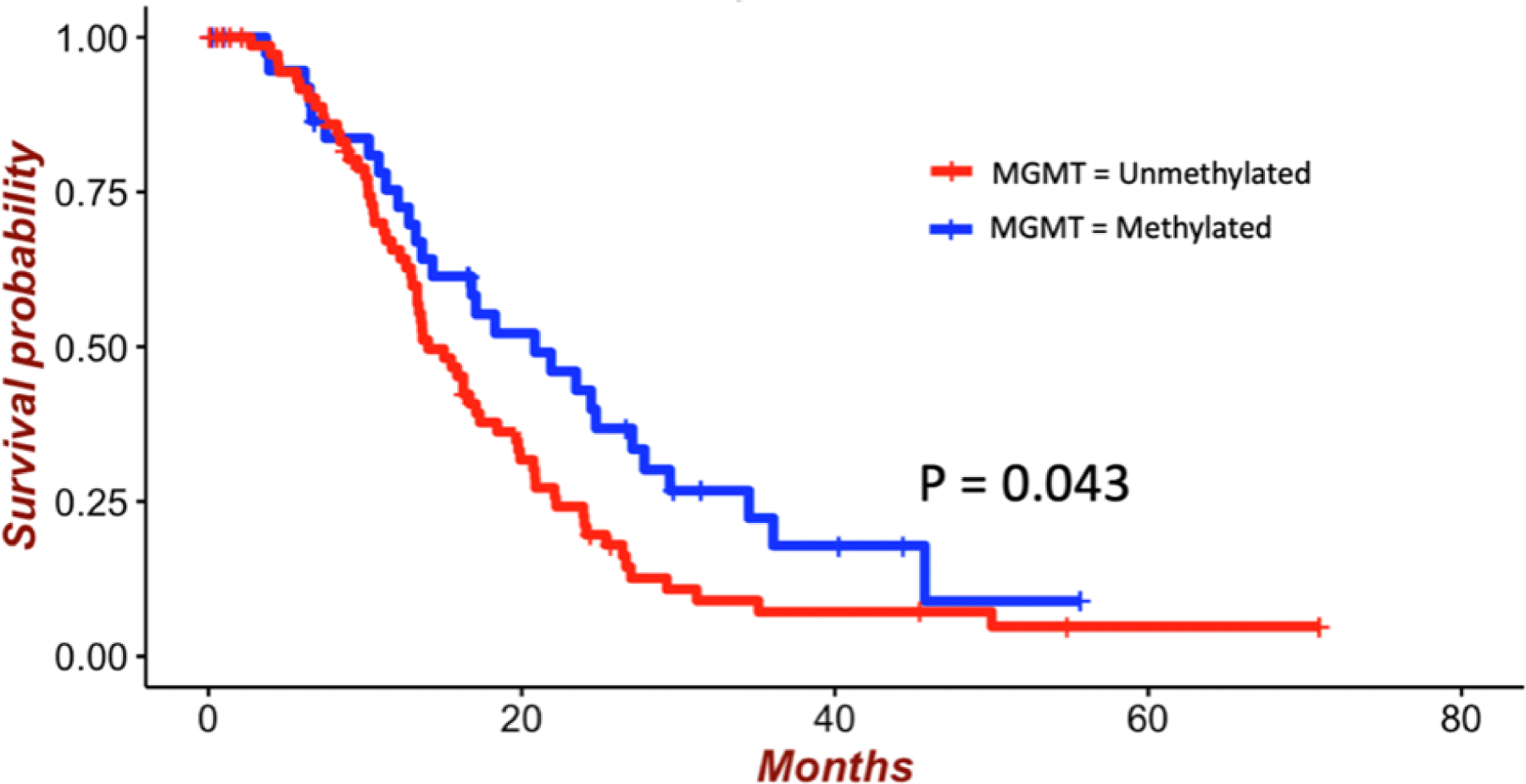
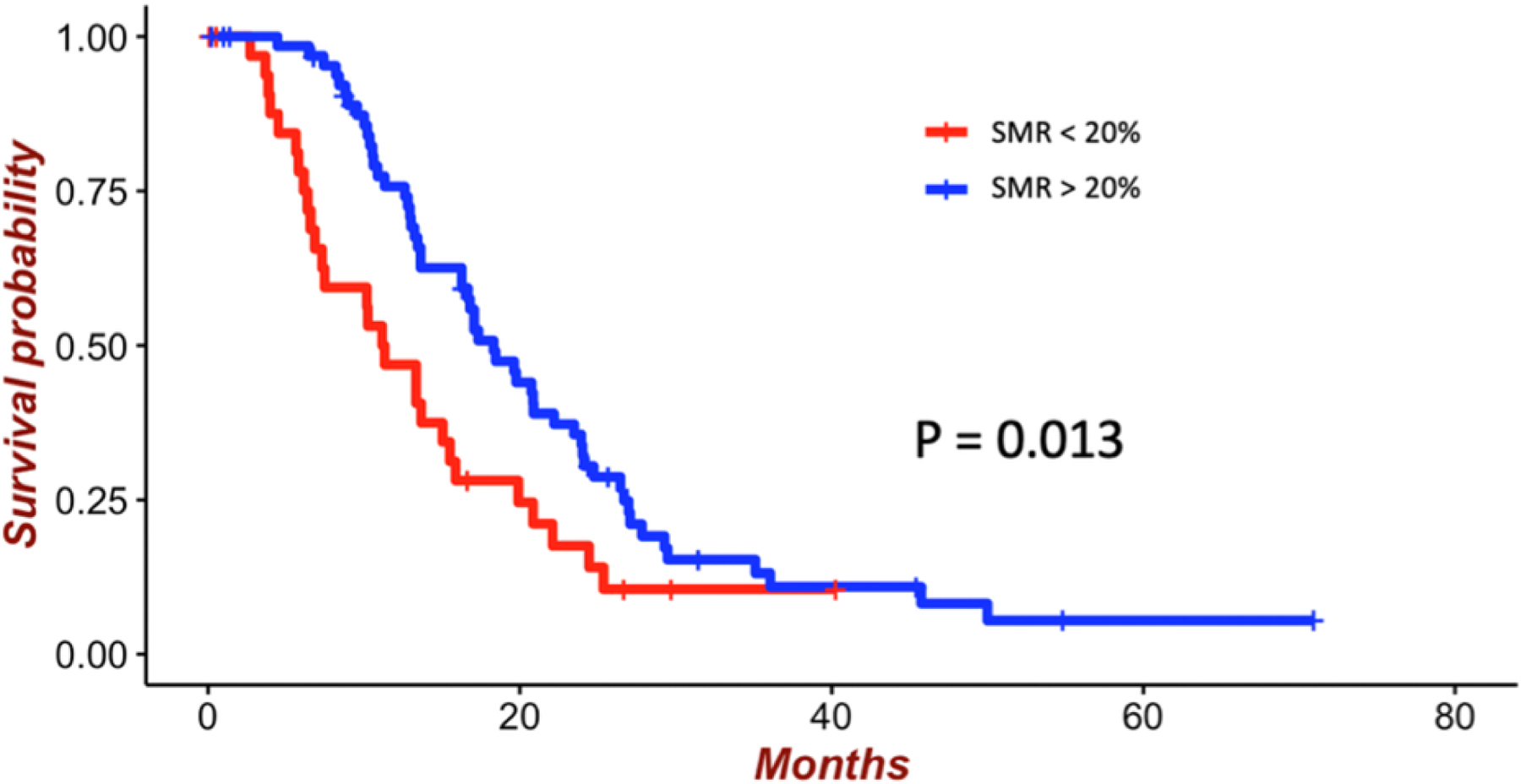
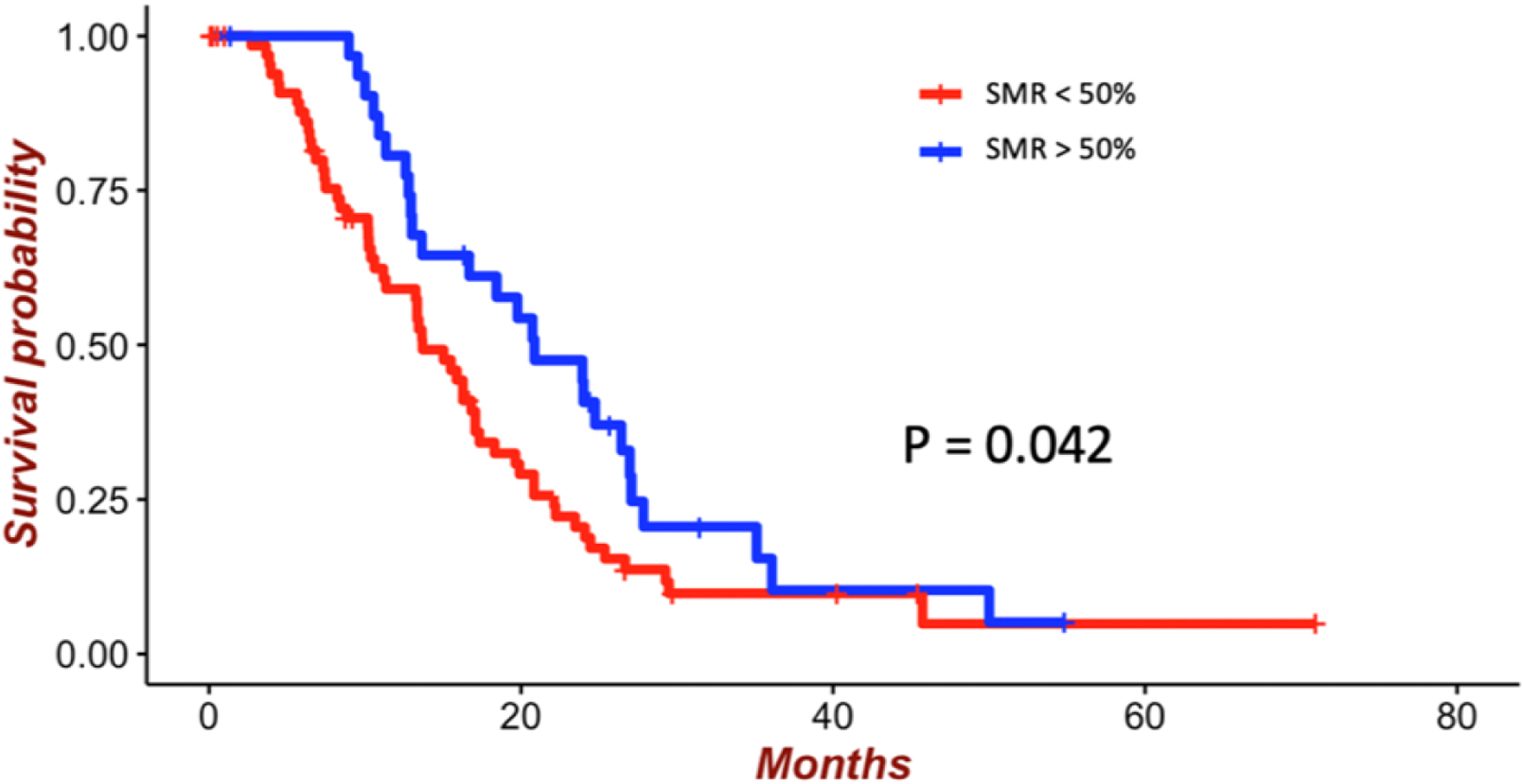
Results: In total, 101 patients with newly diagnosed IDH-wt GBM who underwent GTR of the CE tumor met the inclusion criteria. In multivariate analysis, age ≥ 65 years (HR 1.97; 95% CI 1.01-2.56; p < 0.001) and contact with the lateral ventricles (HR 1.59; 95% CI 1.13-1.78; p = 0.025) were associated with shorter OS, but preoperative Karnofsky Performance Status ≥ 70 (HR 0.47; 95% CI 0.27-0.89; p = 0.006), MGMT promotor methylation (HR 0.63; 95% CI 0.52-0.99; p = 0.044), and increased percentage of SMR (HR 0.99; 95% CI 0.98-0.99; p = 0.02) were associated with longer OS. Finally, 20% SMR was the minimum percentage associated with beneficial OS (HR 0.56; 95% CI 0.35-0.89; p = 0.01), but > 60% SMR had no significant influence (HR 0.74; 95% CI 0.45-1.21; p = 0.234).
Conclusions: SMR is associated with improved OS in patients with IDH-wt GBM who undergo GTR of CE tumor. At least 20% SMR of the CE tumor was associated with beneficial OS, but greater than 60% SMR had no significant influence on OS.
Keywords: FLAIR; IDH–wild type; contrast enhancement; extent of resection; glioblastoma; oncology; supramarginal resection; survival.
Conflict of interest statement
Figures
References
-
- Miranda A, Blanco-Prieto M, Sousa J, Pais A, Vitorino C. Breaching barriers in glioblastoma. Part I: Molecular pathways and novel treatment approaches. Int J Pharm. 2017;531(1):372–388. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
