

Health care cost and benefits of artificial intelligence-assisted population-based glaucoma screening for the elderly in remote areas of China: a cost-offset analysis
- PMID: 34088286
- PMCID: PMC8178835
- DOI: 10.1186/s12889-021-11097-w
Health care cost and benefits of artificial intelligence-assisted population-based glaucoma screening for the elderly in remote areas of China: a cost-offset analysis
Abstract
Background: Population-based screening was essential for glaucoma management. Although various studies have investigated the cost-effectiveness of glaucoma screening, policymakers facing with uncontrollably growing total health expenses were deeply concerned about the potential financial consequences of glaucoma screening. This present study was aimed to explore the impact of glaucoma screening with artificial intelligence (AI) automated diagnosis from a budgetary standpoint in Changjiang county, China.
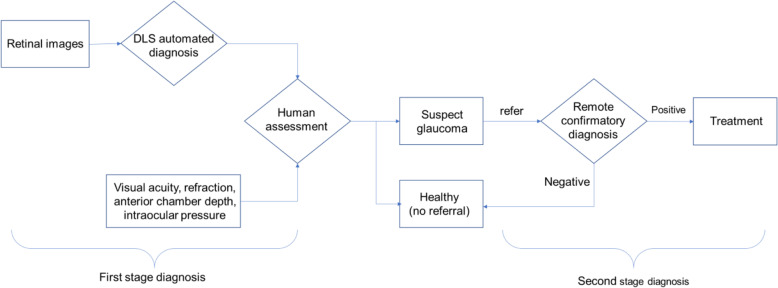
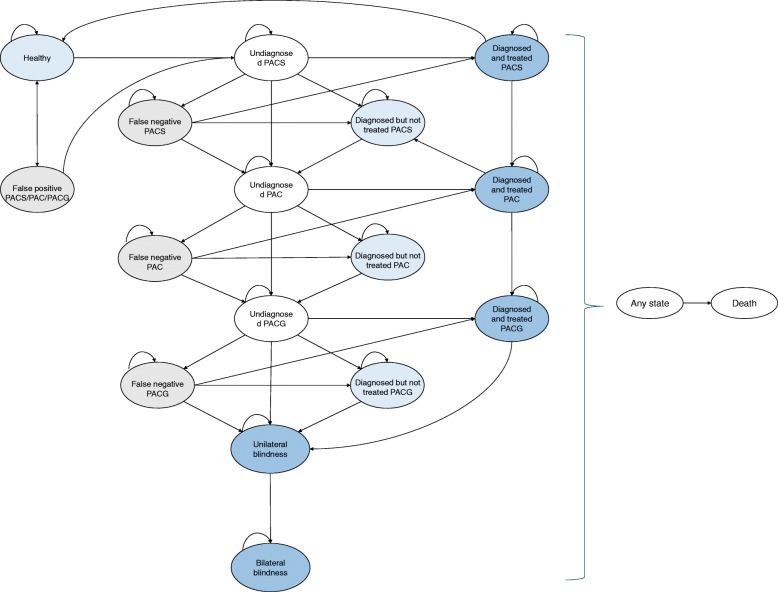
Methods: A Markov model based on health care system's perspective was adapted from previously published studies to predict disease progression and healthcare costs. A cohort of 19,395 individuals aged 65 and above were simulated over a 15-year timeframe. Fur illustrative purpose, we only considered primary angle-closure glaucoma (PACG) in this study. Prevalence, disease progression risks between stages, compliance rates were obtained from publish studies. We did a meta-analysis to estimate diagnostic performance of AI automated diagnosis system from fundus image. Screening costs were provided by the Changjiang screening programme, whereas treatment costs were derived from electronic medical records from two county hospitals. Main outcomes included the number of PACG patients and health care costs. Cost-offset analysis was employed to compare projected health outcomes and medical care costs under the screening with what they would have been without screening. One-way sensitivity analysis was conducted to quantify uncertainties around model results.
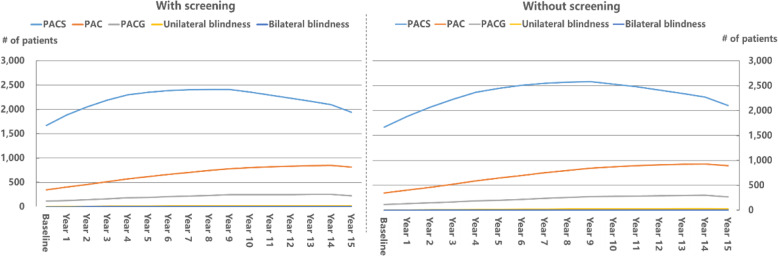
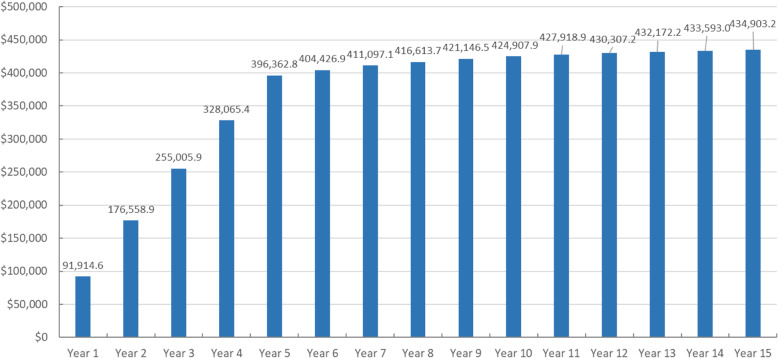
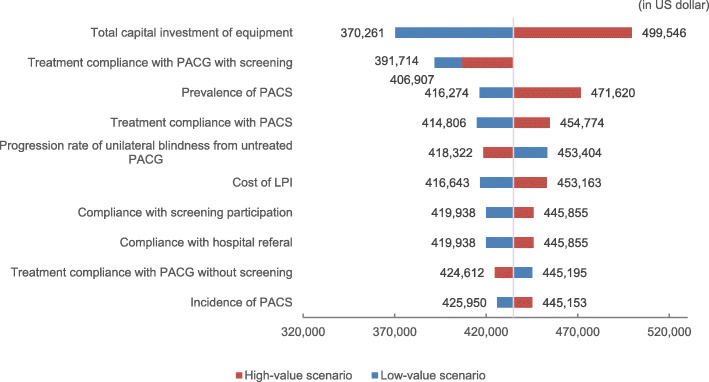
Results: Among people aged 65 and above in Changjiang county, it was predicted that there were 1940 PACG patients under the AI-assisted screening scenario, compared with 2104 patients without screening in 15 years' time. Specifically, the screening would reduce patients with primary angle closure suspect by 7.7%, primary angle closure by 8.8%, PACG by 16.7%, and visual blindness by 33.3%. Due to early diagnosis and treatment under the screening, healthcare costs surged dramatically to $107,761.4 dollar in the first year and then were constantly declining over time, while without screening costs grew from $14,759.8 in the second year until peaking at $17,900.9 in the 9th year. However, cost-offset analysis revealed that additional healthcare costs resulted from the screening could not be offset by decreased disease progression. The 5-, 10-, and 15-year accumulated incremental costs of screening versus no screening were estimated to be $396,362.8, $424,907.9, and $434,903.2, respectively. As a result, the incremental cost per PACG of any stages prevented was $1464.3.
Conclusions: This study represented the first attempt to address decision-maker's budgetary concerns when adopting glaucoma screening by developing a Markov prediction model to project health outcomes and costs. Population screening combined with AI automated diagnosis for PACG in China were able to reduce disease progression risks. However, the excess costs of screening could never be offset by reduction in disease progression. Further studies examining the cost-effectiveness or cost-utility of AI-assisted glaucoma screening were needed.
Keywords: Artificial intelligence (AI); Glaucoma screening; Grassroots community health care; Health economics.
Conflict of interest statement
The authors declare that no competing interests existed.
Figures
Similar articles
-
Cost-effectiveness and cost-utility of population-based glaucoma screening in China: a decision-analytic Markov model.Lancet Glob Health. 2019 Jul;7(7):e968-e978. doi: 10.1016/S2214-109X(19)30201-3. Epub 2019 May 20. Lancet Glob Health. 2019. PMID: 31122906
-
Artificial Intelligence in Community-Based Diabetic Retinopathy Telemedicine Screening in Urban China: Cost-effectiveness and Cost-Utility Analyses With Real-world Data.JMIR Public Health Surveill. 2023 Feb 23;9:e41624. doi: 10.2196/41624. JMIR Public Health Surveill. 2023. PMID: 36821353 Free PMC article.
-
Economic evaluation of combined population-based screening for multiple blindness-causing eye diseases in China: a cost-effectiveness analysis.Lancet Glob Health. 2023 Mar;11(3):e456-e465. doi: 10.1016/S2214-109X(22)00554-X. Epub 2023 Jan 23. Lancet Glob Health. 2023. PMID: 36702141
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
-
Glaucoma screening: where are we and where do we need to go?Curr Opin Ophthalmol. 2020 Mar;31(2):91-100. doi: 10.1097/ICU.0000000000000649. Curr Opin Ophthalmol. 2020. PMID: 31904596 Review.
Cited by
-
Addressing social determinants of health in the field of ophthalmology: In response to: Identifying and addressing social determinants of health to improve patient-centered care - Kalsi N, Gordon D, Geske J.J Clin Transl Sci. 2024 Sep 20;8(1):e130. doi: 10.1017/cts.2024.596. eCollection 2024. J Clin Transl Sci. 2024. PMID: 39345698 Free PMC article. No abstract available.
-
Economic evaluations of artificial intelligence-based healthcare interventions: a systematic literature review of best practices in their conduct and reporting.Front Pharmacol. 2023 Aug 8;14:1220950. doi: 10.3389/fphar.2023.1220950. eCollection 2023. Front Pharmacol. 2023. PMID: 37693892 Free PMC article.
-
Seizing the silent vision loss: cost-utility analysis of population-based glaucoma screening in India.BMJ Open. 2025 Apr 3;15(4):e098113. doi: 10.1136/bmjopen-2024-098113. BMJ Open. 2025. PMID: 40180372 Free PMC article.
-
Glaucoma Screening: Is AI the Answer?J Curr Glaucoma Pract. 2022 May-Aug;16(2):71-73. doi: 10.5005/jp-journals-10078-1380. J Curr Glaucoma Pract. 2022. PMID: 36128081 Free PMC article.
-
Influence of artificial intelligence on ophthalmologists' judgments in glaucoma.PLoS One. 2025 Apr 16;20(4):e0321368. doi: 10.1371/journal.pone.0321368. eCollection 2025. PLoS One. 2025. PMID: 40238811 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
