

Prognostic Significance of Blood-Based Multi-cancer Detection in Plasma Cell-Free DNA
- PMID: 34088722
- PMCID: PMC9401481
- DOI: 10.1158/1078-0432.CCR-21-0417
Prognostic Significance of Blood-Based Multi-cancer Detection in Plasma Cell-Free DNA
Abstract
Purpose: We recently reported the development of a cell-free DNA (cfDNA) targeted methylation (TM)-based sequencing approach for a multi-cancer early detection (MCED) test that includes cancer signal origin prediction. Here, we evaluated the prognostic significance of cancer detection by the MCED test using longitudinal follow-up data.
Experimental design: As part of a Circulating Cell-free Genome Atlas (CCGA) substudy, plasma cfDNA samples were sequenced using a TM approach, and machine learning classifiers predicted cancer status and cancer signal origin. Overall survival (OS) of cancer participants in the first 3 years of follow-up was evaluated in relation to cancer detection by the MCED test and clinical characteristics.
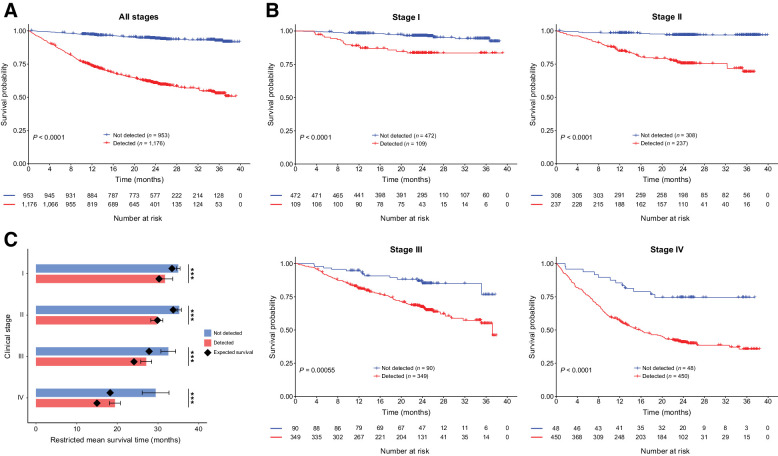
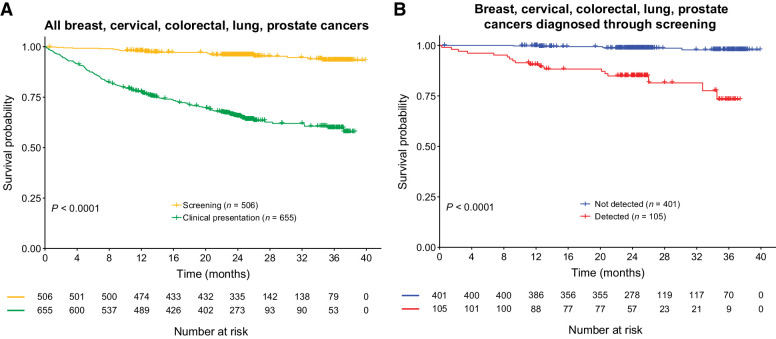
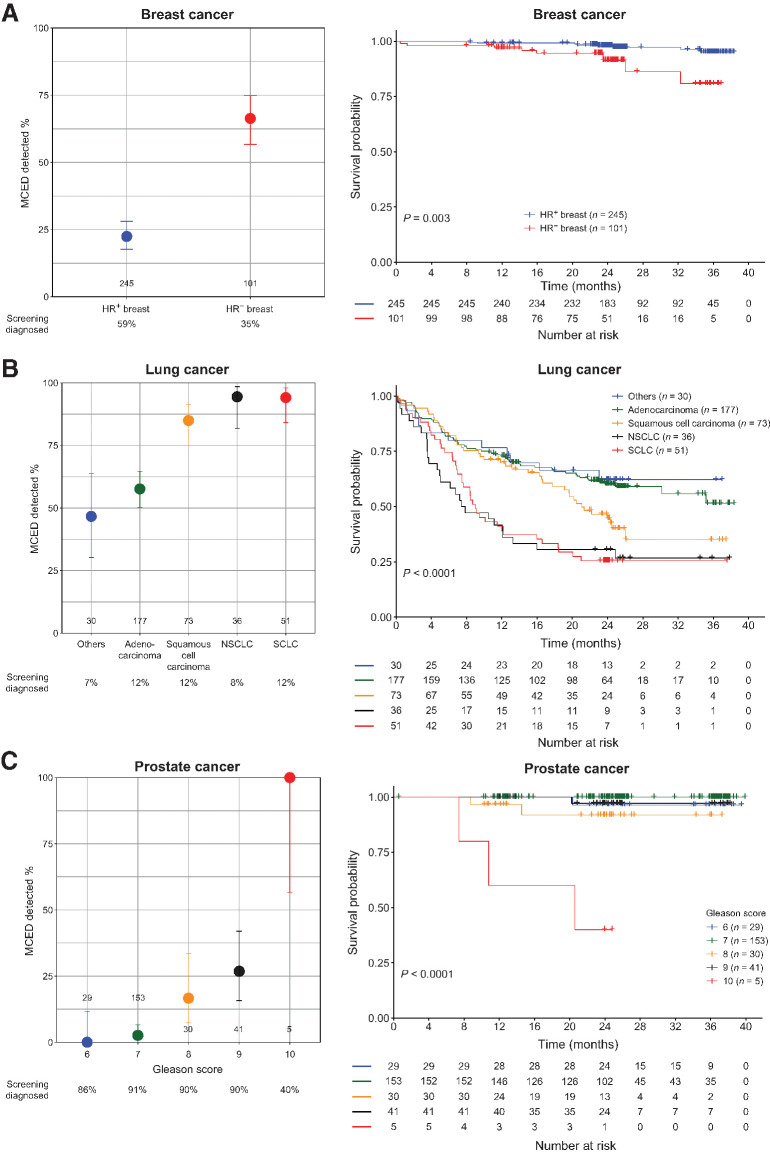
Results: Cancers not detected by the MCED test had significantly better OS (P < 0.0001) than cancers detected, even after accounting for other covariates, including clinical stage and method of clinical diagnosis (i.e., standard-of-care screening or clinical presentation with signs/symptoms). Additionally, cancers not detected by the MCED test had better OS than was expected when data were adjusted for age, stage, and cancer type from the Surveillance, Epidemiology, and End Results (SEER) program. In cancers with current screening options, the MCED test also differentiated more aggressive cancers from less aggressive cancers (P < 0.0001).
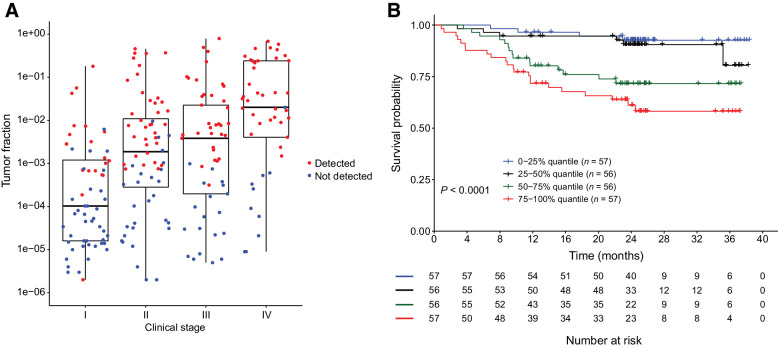
Conclusions: Cancer detection by the MCED test was prognostic beyond clinical stage and method of diagnosis. Cancers not detected by the MCED test had better prognosis than cancers detected and SEER-based expected survival. Cancer detection and prognosis may be linked by the underlying biological factor of tumor fraction in cfDNA.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures
![Figure 2. Multivariate Cox proportional hazards regression model to identify factors associated with OS. Hazard ratios and 95% CIs are indicated by black boxes and gray lines, respectively. P values are indicated. Cancer mortality group is based on SEER 5-year survival of stage II cancers. Cancer mortality hazard-high group includes sarcoma, head and neck, cervix, plasma cell neoplasm, urothelial tract, bladder, myeloid neoplasm, stomach, lung, liver bile duct, esophagus, gallbladder, and pancreas cancer types. Cancer mortality hazard-low group includes thyroid, prostate, breast, kidney, uterus, lymphoid leukemia, lymphoma, ovary, colon/rectum, anus, melanoma, and other [includes brain, mesothelioma, orbit, penis, pleura, skin cancer (not basal cell carcinoma, squamous cell carcinoma, or melanoma), small intestine, testis, thymus, vagina, vulva, and unspecified] cancer types.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/b12e/9401481/5f0ea1956e8d/4221fig2.jpg)
Comment in
-
Prognostic significance of blood-based multi-cancer detection in plasma cell-free DNA.Clin Chem Lab Med. 2021 Dec 30;60(3):88-89. doi: 10.1515/cclm-2021-1113. Print 2022 Feb 23. Clin Chem Lab Med. 2021. PMID: 34964568 No abstract available.
References
-
- Chen X, Chang C-W, Spoerke JM, Yoh KE, Kapoor V, Baudo C, et al. . Low-pass whole-genome sequencing of circulating cell-free DNA demonstrates dynamic changes in genomic copy number in a squamous lung cancer clinical cohort. Clin Cancer Res 2019;25:2254–63. - PubMed
-
- Chen L, Zhang Y, Cheng Y, Zhang D, Zhu S, Ma X. Prognostic value of circulating cell-free DNA in patients with pancreatic cancer: a systemic review and meta-analysis. Gene 2018;679:328–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
