

Locked fracture dislocations of the proximal humerus: postoperative results and a proposed modification of the classification
- PMID: 34089131
- PMCID: PMC9001205
- DOI: 10.1007/s00590-021-03022-z
Locked fracture dislocations of the proximal humerus: postoperative results and a proposed modification of the classification
Abstract
Background: Locked dislocations of the glenohumeral joint are disabling and often painful conditions and the treatment is challenging. This study evaluates the functional outcome and the different prosthetic treatment options for chronic locked dislocations of the glenohumeral joint and a subclassification is proposed.
Methods: In this single-center retrospective case series, all patients with a chronic locked dislocation treated surgically during a four-year period were analyzed. Constant score (CS), Quick Disabilities of Shoulder and Hand Score (DASH), patient satisfaction (subjective shoulder value (SSV)), revision rate and glenoid notching were analyzed.
Results: 26 patients presented a chronic locked dislocation of the glenohumeral joint. 16 patients (62%) with a mean age of 75 [61-83] years were available for follow-up at 24 ± 18 months. CS improved significantly from 10 ± 6 points to 58 ± 21 points (p < 0.0001). At the final follow-up, the mean DASH was 27 ± 23 and the mean SSV was 58 ± 23 points. The complication rate was 19% and the revision rate was 6%; implant survival was 94%. Scapular notching occurred in 2 (13%) cases (all grade 1).
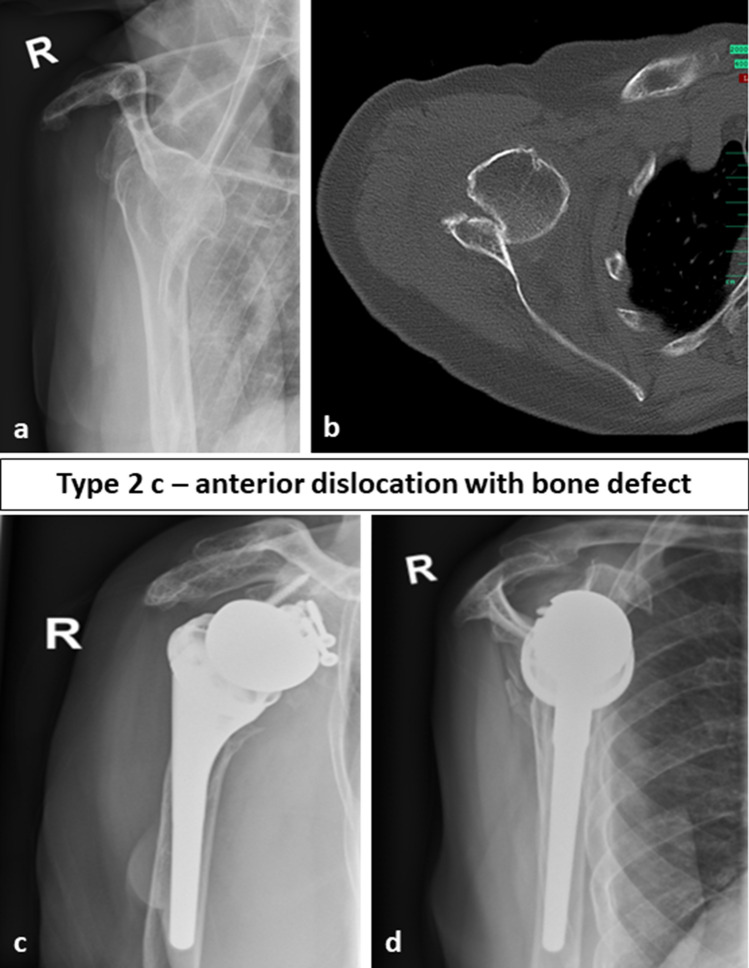
Conclusion: With good preoperative planning and by using the adequate surgical technique, good clinical short-term results with a low revision rate can be achieved. The authors suggest extending the Boileau classification for fracture sequelae type 2 and recommend using a modified classification to facilitate the choice of treatment as the suggested classification system includes locked posterior and anterior dislocations with and without glenoid bone loss.
Level of evidence: IV.
Keywords: Bone defect; Fracture sequelae shoulder; Glenoid bone grafting; Locked shoulder dislocation; Pectoralis major transfer; Shoulder arthroplasty.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures




References
-
- Boileau P, Trojani C, Chuinard C, Lehuec JC, Walch G (2006) Proximal humerus fracture sequelae: impact of a new radiographic classification on arthroplasty. Clin Orthop Relat Res 442:121–130. 10.1097/01.blo.0000195679.87258.6e - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
