

Computed tomography imaging of septic shock. Beyond the cause: the "CT hypoperfusion complex". A pictorial essay
- PMID: 34089401
- PMCID: PMC8178660
- DOI: 10.1186/s13244-021-01006-5
Computed tomography imaging of septic shock. Beyond the cause: the "CT hypoperfusion complex". A pictorial essay
Abstract
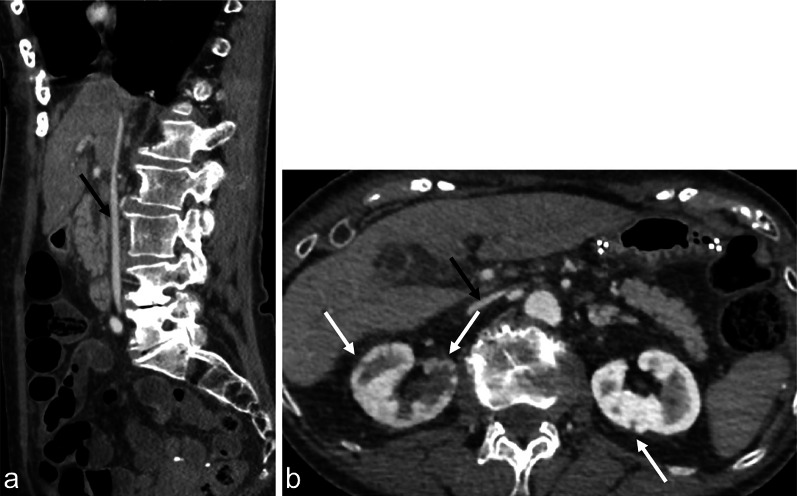
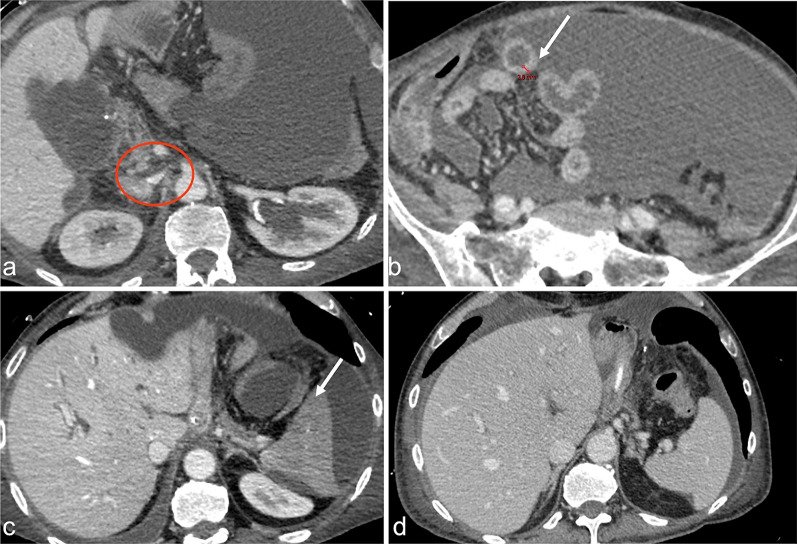
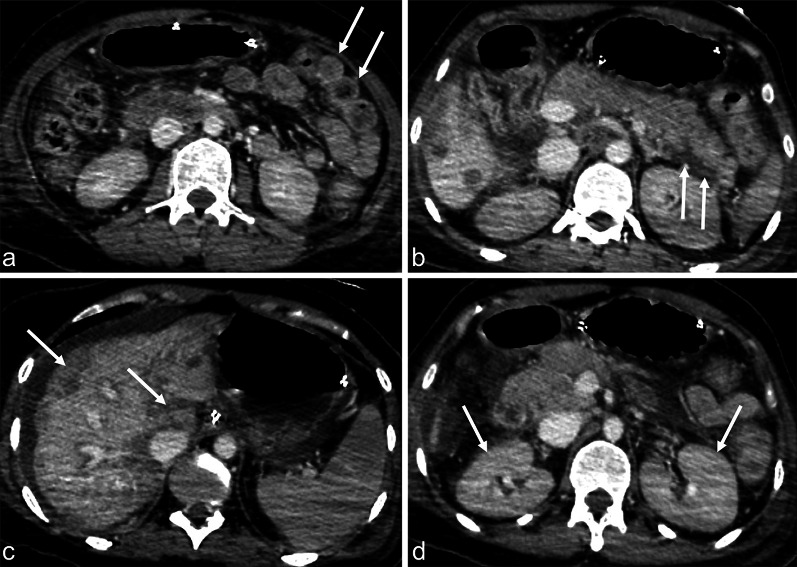
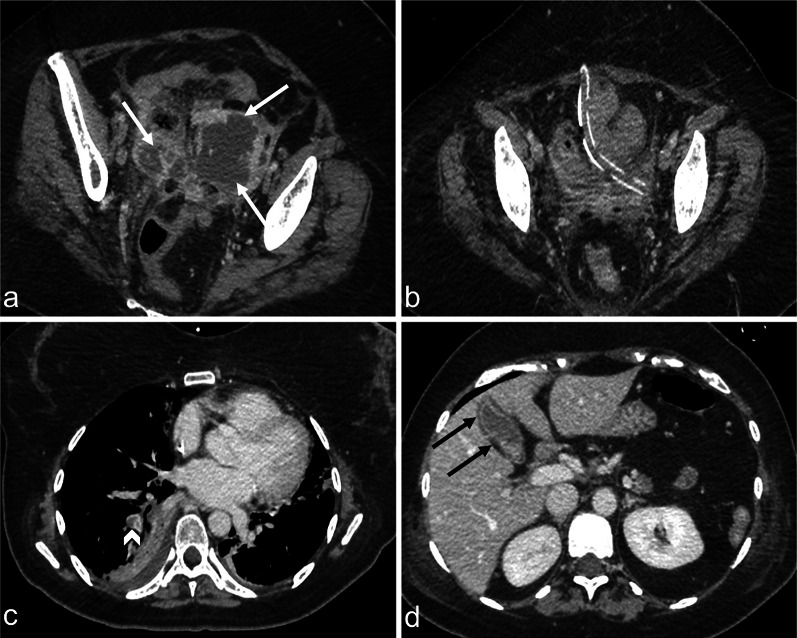
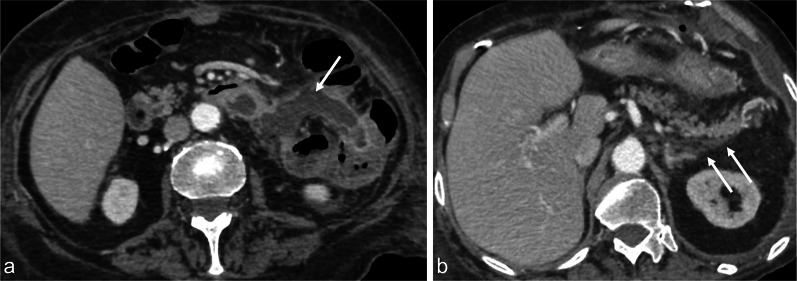
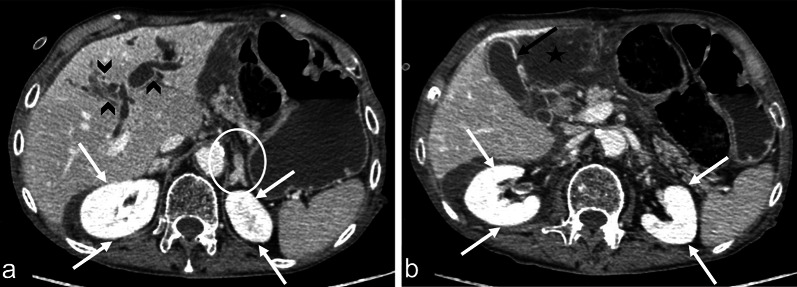
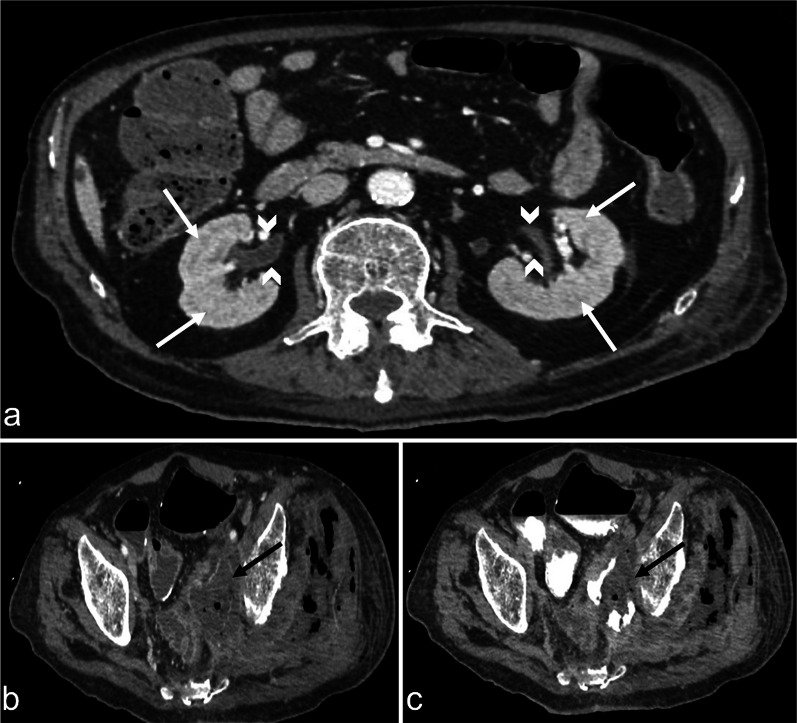
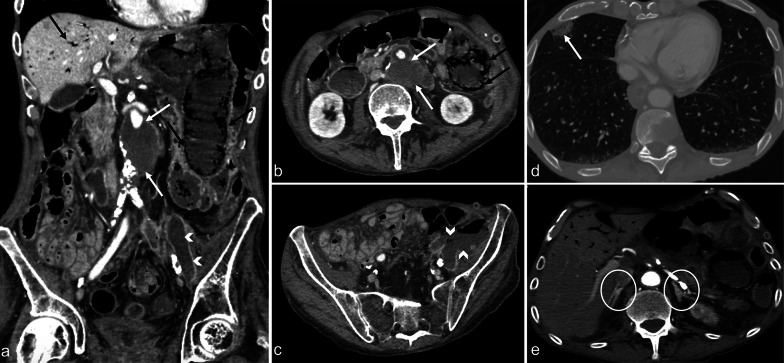
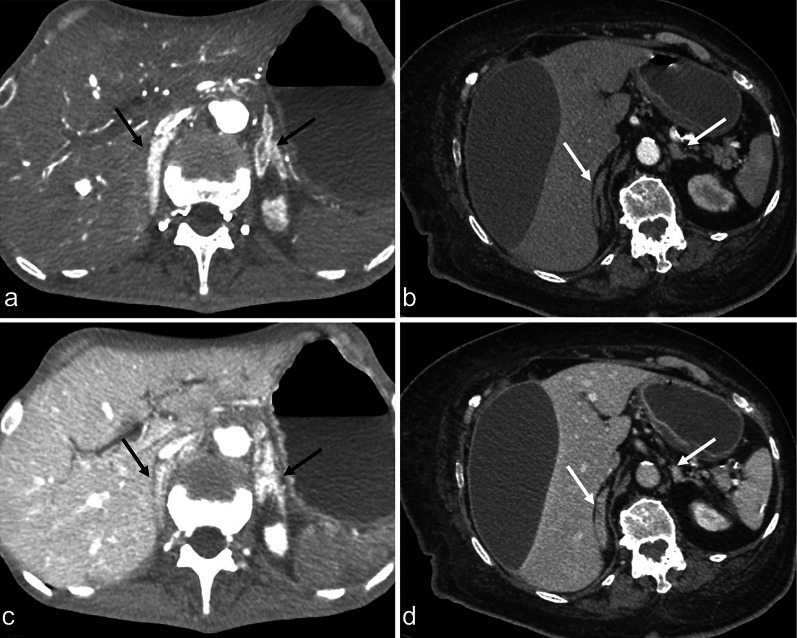
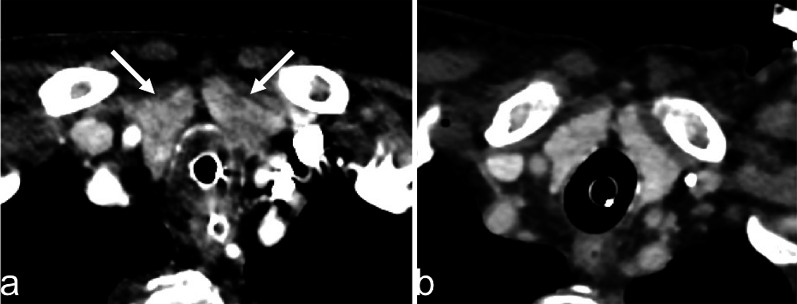
Septic shock is a medical emergency that represents one of the most important underlying causes for presentation to the Emergency Department. Sepsis is defined as organ dysfunction, life-threatening event caused by a deregulated inflammatory host response to infection, with a mortality risk ranging from 10 to 40%. Early sepsis identification is the cornerstone of management and diagnostic imaging can play a pivotal role in this clinical context. The choice of imaging modality depends on several factors, associated with the clinical condition and the presence or absence of localising signs and symptoms. The diagnostic accuracy of contrast-enhanced total-body CT has been well established during septic shock, allowing for a rapid, panoramic, and detailed study of multiple body areas, simultaneously. The aim of this article is to illustrate the controversial CT hypoperfusion complex in patients with septic shock, characterised by the following imaging features: decreased enhancement of the viscera; increased mucosal enhancement; luminal dilation of the small bowel; mural thickening and fluid-filled loops of the small bowel; the halo sign and flattening of the inferior vena cava; reduced aortic diameter; peripancreatic oedema; abnormal parenchymal perfusion; and other controversial findings that are variably associated with each other and reversible during the early stages. Increasing physicians' awareness of the significance of these findings could prompt alternative approaches to the early assessment and management of septic shock. In this perspective, CT imaging represents a useful tool for a complete, rapid and detailed diagnosis of clinically suspected septic shock, which can be used to improve patient outcomes.
Keywords: CT hypoperfusion complex; Contrast-enhanced CT; Diagnostic imaging; Sepsis; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):775–787. doi: 10.1001/jama.2016.0289. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
