

Impact of Changes in Free Concentrations and Drug-Protein Binding on Drug Dosing Regimens in Special Populations and Disease States
- PMID: 34089711
- PMCID: PMC8458247
- DOI: 10.1016/j.xphs.2021.05.018
Impact of Changes in Free Concentrations and Drug-Protein Binding on Drug Dosing Regimens in Special Populations and Disease States
Abstract
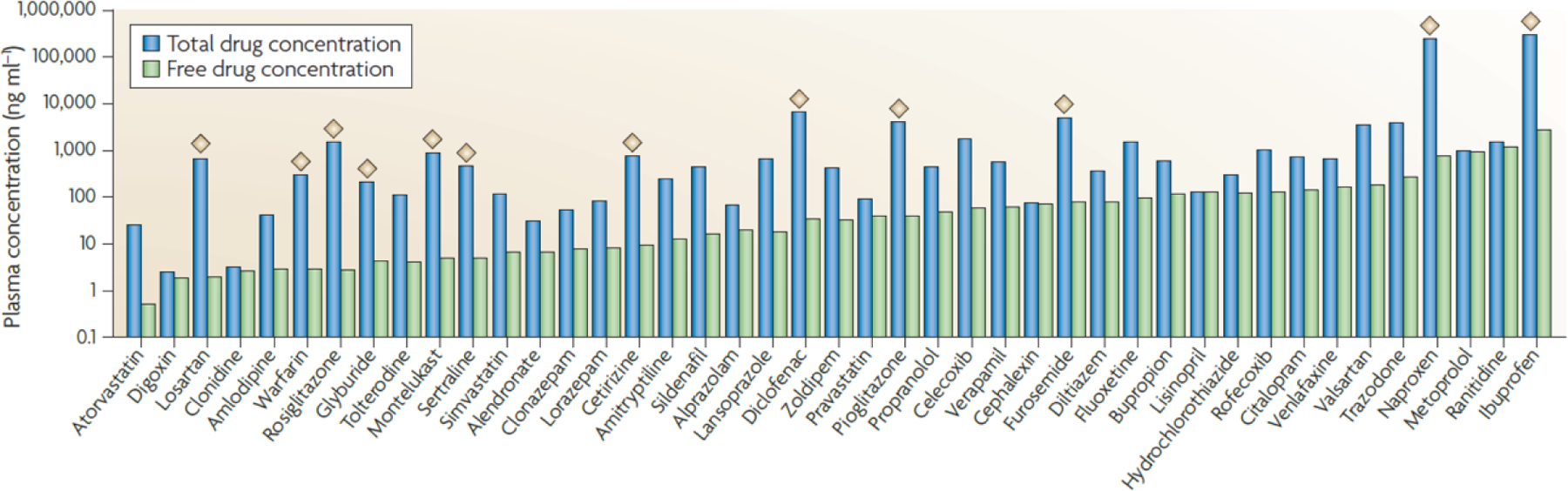
Over the last few decades, scientists and clinicians have often focused their attention on the unbound fraction of drugs as an indicator of efficacy and the eventual outcome of drug treatments for specific illnesses. Typically, the total drug concentration (bound and unbound) in plasma is used in clinical trials to assess a compound's efficacy. However, the free concentration of a drug tends to be more closely related to its activity and interaction with the body. Thus far, measuring the unbound concentration has been a challenge. Several mechanistic models have attempted to solve this problem by estimating the free drug fraction from available data such as total drug and binding protein concentrations. The aims of this review are first, to give an overview of the methods that have been used to date to calculate the unbound drug fraction. Second, to assess the pharmacokinetic parameters affected by changes in drug protein binding in special populations such as pediatrics, the elderly, pregnancy, and obesity. Third, to review alterations in drug protein binding in some selected disease states and how these changes impact the clinical outcomes for the patients; the disease states include critical illnesses, transplantation, renal failure, chronic kidney disease, and epilepsy. And finally, to discuss how various disease states shift the ratio of unbound to total drug and the consequences of such shifts on dosing adjustments and reaching the therapeutic target.
Keywords: Disease state(s); Dose-response; Drug distribution; Drug transport; Protein binding; Special populations.
Copyright © 2021 American Pharmacists Association. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declarations of Competing Interest None.
Figures
References
-
- Musteata FM 2012. Calculation of Normalized Drug Concentrations in the Presence of Altered Plasma Protein Binding. Clin Pharmacokinet 51(1):55–68. - PubMed
-
- Smith DA, Di L, Kerns EH 2010. The effect of plasma protein binding on in vivo efficacy: misconceptions in drug discovery. Nat Rev Drug Discov 9(12):929–939. - PubMed
-
- Bohnert T, Gan LS 2013. Plasma Protein Binding: From Discovery to Development. J Pharm Sci 102(9):2953–2994. - PubMed
-
- Roberts JA, Pea F, Lipman J 2013. The Clinical Relevance of Plasma Protein Binding Changes. Clin Pharmacokinet 52(1):1–8. - PubMed
-
- Benet LZ, Hoener BA 2002. Changes in plasma protein binding have little clinical relevance. Clin Pharmacol Ther 71(3):115–121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
