

Iron metabolism: pathophysiology and pharmacology
- PMID: 34090703
- PMCID: PMC7611894
- DOI: 10.1016/j.tips.2021.05.001
Iron metabolism: pathophysiology and pharmacology
Abstract
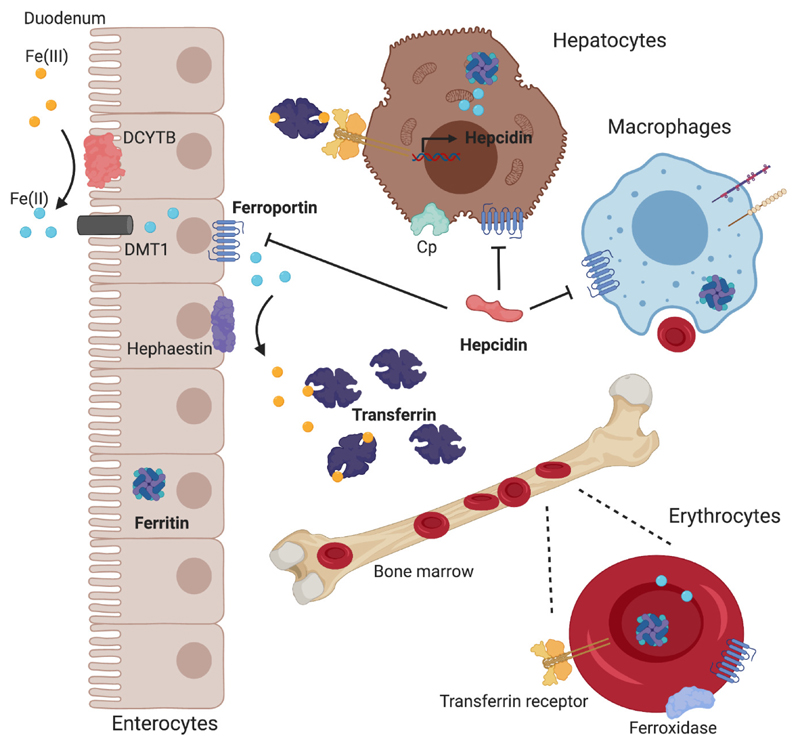
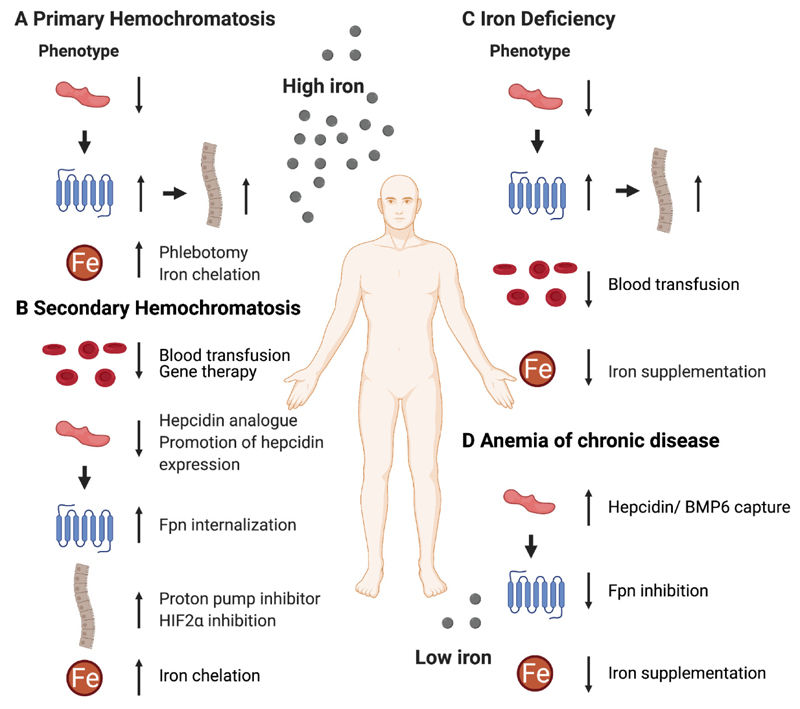
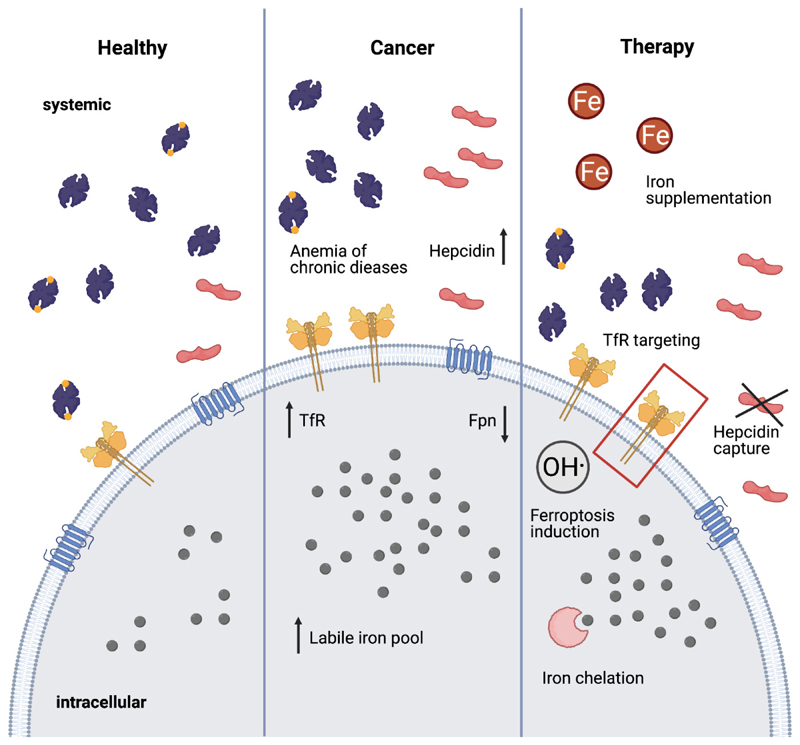
Iron is essential in many physiological processes, including DNA metabolism, oxygen transport, and cellular energy generation. Deregulated iron metabolism, which results in iron overload or iron deficiency, is observed in many different diseases. We here summarize recent progress in the pathophysiology and pharmacology of iron-overload diseases, such as hereditary hemochromatosis, as well as iron-deficiency disorders, which are typically associated with anemia. The role of iron in immunity and the connection between iron and cancer are also addressed. We finally summarize and discuss the current (pre-) clinical landscape of pharmacotherapies targeting key players involved in iron metabolism.
Keywords: anemia; cancer; hemochromatosis; inflammation; iron.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests All authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
