

Acquired antithrombin deficiency is a risk factor for venous thromboembolism after major trauma
- PMID: 34091120
- PMCID: PMC9653093
- DOI: 10.1016/j.thromres.2021.05.015
Acquired antithrombin deficiency is a risk factor for venous thromboembolism after major trauma
Abstract
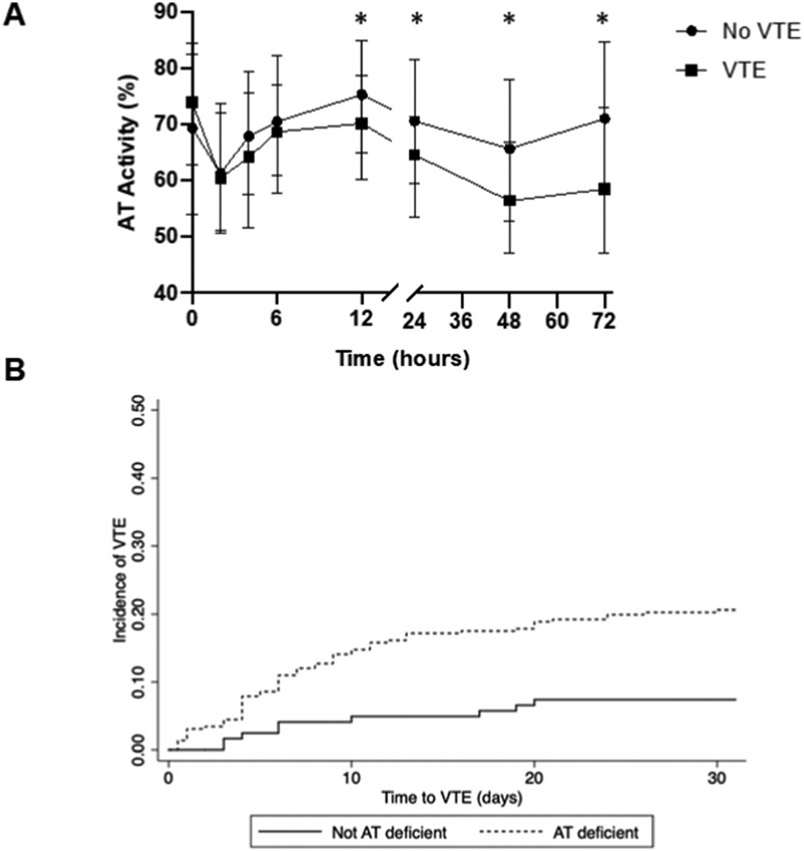
Background: Up to 30% of severely injured patients on prophylactic anticoagulation experience venous thromboembolism (VTE). Our previous work shows that acquired antithrombin (AT) deficiency [AT<80%] occurs in approximately 20% of trauma patients upon admission and drives poor responsiveness to enoxaparin. However, changes in AT over time and its association with VTE remain unknown. The aim of this study was to determine the relationship between acquired AT deficiency and VTE in severely injured patients.
Methods: A secondary analysis of the Pragmatic, Randomized Optimal Platelet and Plasma Ratios (PROPPR) clinical trial was performed. Patients who died within 24 h of hemorrhage were excluded from analysis. Demographics, mechanism and severity of injury, transfusions volumes, and outcomes were compared between patients who did and did not develop VTE. Non-parametric statistical tests were used to compare patients with and without VTE. Logistic regression analyses were performed to identify predictors of VTE risk, controlling for AT deficiency (over first 72 h), age, gender, race, body mass index, study site, randomization group and injury severity. A Cox proportional hazards model was used to assess the contribution of AT deficiency to the risk of VTE, while censoring for early deaths.
Results: Of the 680 patients enrolled in PROPPR, 101 died of hemorrhage. Of the remaining 579 patients, 86 (14.9%) developed VTE. The median time to VTE was 6 days (IQR 3, 13). No differences in demographics, injuries, or transfusion volumes were identified between VTE cases and controls. AT deficiency at 72 h post-admission was independently associated with VTE. Patients who experienced AT deficiency at 72 h had a 3.3 fold increased risk of VTE [p < 0.01; 95% CI 1.56, 6.98]. Lastly, patients who developed VTE had worse outcomes as displayed by significantly fewer hospital-free days compared to non-VTE patients [0 (0, 8) vs. 4 (0, 18), p < 0.01, respectively].
Conclusions: Acquired AT deficiency (AT<80%) is an important risk factor for VTE in severely injured patients. These data indicate that intervening, perhaps through AT supplementation, in the first three days after injury could mitigate the risk of VTE and improve patient outcomes.
Keywords: Anticoagulation; Antithrombin; Injury; Thrombosis; Trauma; Venous thromboembolism.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
-
- Drake SA, Holcomb JB, Yang Y, Thetford C, Myers L, Brock M, Wolf DA, Cron S, Persse D, McCarthy J, Kao L, Todd SR, Naik-Mathuria BJ, Cox C, Kitagawa R, Sandberg G, Wade CE, Establishing a regional trauma preventable/potentially preventable death rate, Ann. Surg 271 (2) (2020) 375–382. - PubMed
-
- Meissner MH, Wakefield TW, Ascher E, Caprini JA, Comerota AJ, Eklof B, Gillespie DL, Greenfield LJ, He AR, Henke PK, Hingorani A, Hull RD, Kessler CM, McBane RD, McLafferty R, Acute venous disease: venous thrombosis and venous trauma, J Vasc Surg 46 Suppl S (2007) 25S–53S. - PubMed
-
- Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, Colwell CW, Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition), Chest 133 (6 Suppl) (2008) 381S–453S. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
