

Stratified delirium risk using prescription medication data in a state-wide cohort
- PMID: 34091195
- PMCID: PMC8249339
- DOI: 10.1016/j.genhosppsych.2021.05.001
Stratified delirium risk using prescription medication data in a state-wide cohort
Abstract
Objective: Delirium is a common condition associated with increased morbidity and mortality. Medication side effects are a possible source of modifiable delirium risk and provide an opportunity to improve delirium predictive models. This study characterized the risk for delirium diagnosis by applying a previously validated algorithm for calculating central nervous system adverse effect burden arising from a full medication list.
Method: Using a cohort of hospitalized adult (age 18-65) patients from the Massachusetts All-Payers Claims Database, we calculated medication burden following hospital discharge and characterized risk of new coded delirium diagnosis over the following 90 days. We applied the resulting model to a held-out test cohort.
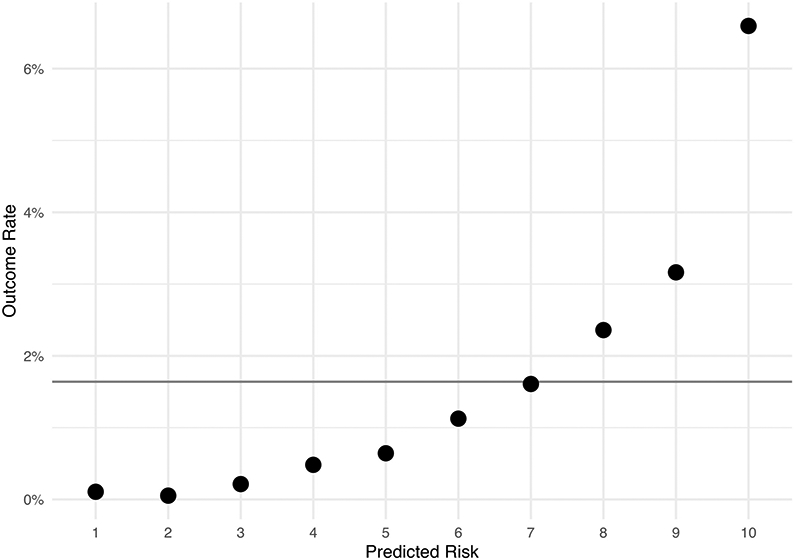
Results: The cohort included 62,180 individuals of whom 1.6% (1019) went on to have a coded delirium diagnosis. In the training cohort (43,527 individuals), the medication burden feature was positively associated with delirium diagnosis (OR = 5.75, 95% CI 4.34-7.63) and this association persisted (aOR = 1.95; 1.31-2.92) after adjusting for demographics, clinical features, prescribed medications, and anticholinergic risk score. In the test cohort, the trained model produced an area under the curve of 0.80 (0.78-0.82). This performance was similar across subgroups of age and gender.
Conclusion: Aggregating brain-related medication adverse effects facilitates identification of individuals at high risk of subsequent delirium diagnosis.
Keywords: Cohort study; Data mining; Delirium; Feature engineering; Pharmacovigilance; Predictive modeling.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Relation Between Delirium and Anticholinergic Drug Burden in a Cohort of Hospitalized Older Patients: An Observational Study.Drugs Aging. 2019 Jan;36(1):85-91. doi: 10.1007/s40266-018-0612-9. Drugs Aging. 2019. PMID: 30484239
-
Associations between Anticholinergic Burden and Adverse Health Outcomes in Parkinson Disease.PLoS One. 2016 Mar 3;11(3):e0150621. doi: 10.1371/journal.pone.0150621. eCollection 2016. PLoS One. 2016. PMID: 26939130 Free PMC article.
-
Anticholinergic Medication Burden in Pediatric Prolonged Critical Illness: A Potentially Modifiable Risk Factor for Delirium.Pediatr Crit Care Med. 2018 Oct;19(10):917-924. doi: 10.1097/PCC.0000000000001658. Pediatr Crit Care Med. 2018. PMID: 30284995 Free PMC article.
-
[Drug-induced delirium].Ther Umsch. 2010 Feb;67(2):79-83. doi: 10.1024/0040-5930/a000015. Ther Umsch. 2010. PMID: 20131216 Review. German.
-
Are potentially inappropriate and anticholinergic medications being prescribed for institutionalized elderly subjects?Fundam Clin Pharmacol. 2020 Dec;34(6):743-748. doi: 10.1111/fcp.12560. Epub 2020 May 17. Fundam Clin Pharmacol. 2020. PMID: 32289182 Review.
Cited by
-
Development and validation of a new drug-focused predictive risk score for postoperative delirium in orthopaedic and trauma surgery patients.BMC Geriatr. 2024 May 13;24(1):422. doi: 10.1186/s12877-024-05005-1. BMC Geriatr. 2024. PMID: 38741037 Free PMC article.
-
Real-world evidence of age-independent electroconvulsive therapy efficacy: A retrospective cohort study.Acta Psychiatr Scand. 2022 Jan;145(1):100-108. doi: 10.1111/acps.13378. Epub 2021 Oct 25. Acta Psychiatr Scand. 2022. PMID: 34662429 Free PMC article.
-
Use of a Data Repository to Identify Delirium as a Presenting Symptom of COVID-19 Infection in Hospitalized Adults: Cross-Sectional Cohort Pilot Study.JMIR Aging. 2023 Nov 30;6:e43185. doi: 10.2196/43185. JMIR Aging. 2023. PMID: 37910448 Free PMC article.
-
Longitudinal validation of an electronic health record delirium prediction model applied at admission in COVID-19 patients.Gen Hosp Psychiatry. 2022 Jan-Feb;74:9-17. doi: 10.1016/j.genhosppsych.2021.10.005. Epub 2021 Nov 2. Gen Hosp Psychiatry. 2022. PMID: 34798580 Free PMC article.
References
-
- Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, D.C.: American Psychiatric Association; 2013.
-
- Inouye SK, Charpentier PA Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 1996;275:852–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
