

Clinical presentation of new onset refractory status epilepticus in children (the pSERG cohort)
- PMID: 34091885
- PMCID: PMC8362203
- DOI: 10.1111/epi.16950
Clinical presentation of new onset refractory status epilepticus in children (the pSERG cohort)
Abstract
Objective: We aimed to characterize the clinical profile and outcomes of new onset refractory status epilepticus (NORSE) in children, and investigated the relationship between fever onset and status epilepticus (SE).
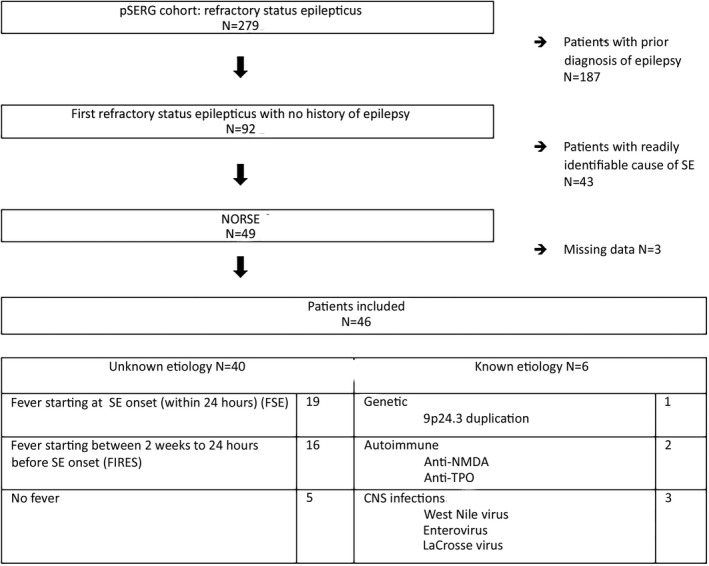
Methods: Patients with refractory SE (RSE) between June 1, 2011 and October 1, 2016 were prospectively enrolled in the pSERG (Pediatric Status Epilepticus Research Group) cohort. Cases meeting the definition of NORSE were classified as "NORSE of known etiology" or "NORSE of unknown etiology." Subgroup analysis of NORSE of unknown etiology was completed based on the presence and time of fever occurrence relative to RSE onset: fever at onset (≤24 h), previous fever (2 weeks-24 h), and without fever.
Results: Of 279 patients with RSE, 46 patients met the criteria for NORSE. The median age was 2.4 years, and 25 (54%) were female. Forty (87%) patients had NORSE of unknown etiology. Nineteen (48%) presented with fever at SE onset, 16 (40%) had a previous fever, and five (12%) had no fever. The patients with preceding fever had more prolonged SE and worse outcomes, and 25% recovered baseline neurological function. The patients with fever at onset were younger and had shorter SE episodes, and 89% recovered baseline function.
Significance: Among pediatric patients with RSE, 16% met diagnostic criteria for NORSE, including the subcategory of febrile infection-related epilepsy syndrome (FIRES). Pediatric NORSE cases may also overlap with refractory febrile SE (FSE). FIRES occurs more frequently in older children, the course is usually prolonged, and outcomes are worse, as compared to refractory FSE. Fever occurring more than 24 h before the onset of seizures differentiates a subgroup of NORSE patients with distinctive clinical characteristics and worse outcomes.
Keywords: clinical neurology; epilepsy; febrile infection-related epilepsy syndrome; new onset refractory status epilepticus; pediatric; refractory status epilepticus; status epilepticus.
© 2021 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
C.S. is funded by the International Federation of Clinical Neurophysiology. C.B.A. is funded by the Fundación Alfonso Martín Escudero. I.S.F. is funded by the Epilepsy Research Fund and was funded by the Fundación Alfonso Martín Escudero and the HHV6 Foundation. M.A.‐G. was funded by the Fundación Alfonso Martín Escudero. J.N.B. is funded by National Institutes of Health (NIH) National Institute of Neurological Disorders and Stroke 1K23NS116225. He also served as a consultant for Novartis. W.D.G. is an editor for
Figures
References
-
- Hirsch LJ, Gaspard N, van Baalen A, Nabbout R, Demeret S, Loddenkemper T, et al. Proposed consensus definitions for new‐onset refractory status epilepticus (NORSE), febrile infection‐related epilepsy syndrome (FIRES), and related conditions. Epilepsia. 2018;59(4):739–44. - PubMed
-
- Costello DJ, Kilbride RD, Cole AJ. Cryptogenic new onset refractory status epilepticus (NORSE) in adults—infectious or not? J Neurol Sci. 2009;277(1–2):26–31. - PubMed
-
- Khawaja AM, DeWolfe JL, Miller DW, Szaflarski JP. New‐onset refractory status epilepticus (NORSE)—the potential role for immunotherapy. Epilepsy Behav. 2015;47:17–23. - PubMed
-
- Gall CRE, Jumma O, Mohanraj R. Five cases of new onset refractory status epilepticus (NORSE) syndrome: outcomes with early immunotherapy. Seizure. 2013;22(3):217–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
