

Prognostic Utility of Risk Enhancers and Coronary Artery Calcium Score Recommended in the 2018 ACC/AHA Multisociety Cholesterol Treatment Guidelines Over the Pooled Cohort Equation: Insights From 3 Large Prospective Cohorts
- PMID: 34092110
- PMCID: PMC8477885
- DOI: 10.1161/JAHA.120.019589
Prognostic Utility of Risk Enhancers and Coronary Artery Calcium Score Recommended in the 2018 ACC/AHA Multisociety Cholesterol Treatment Guidelines Over the Pooled Cohort Equation: Insights From 3 Large Prospective Cohorts
Abstract
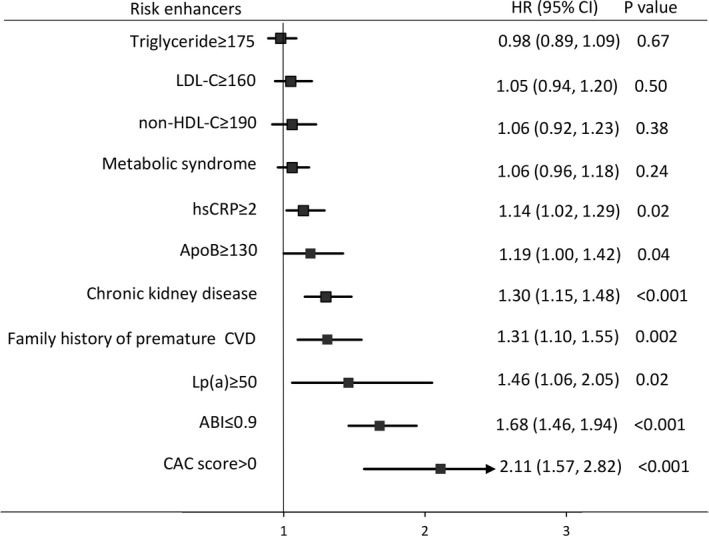
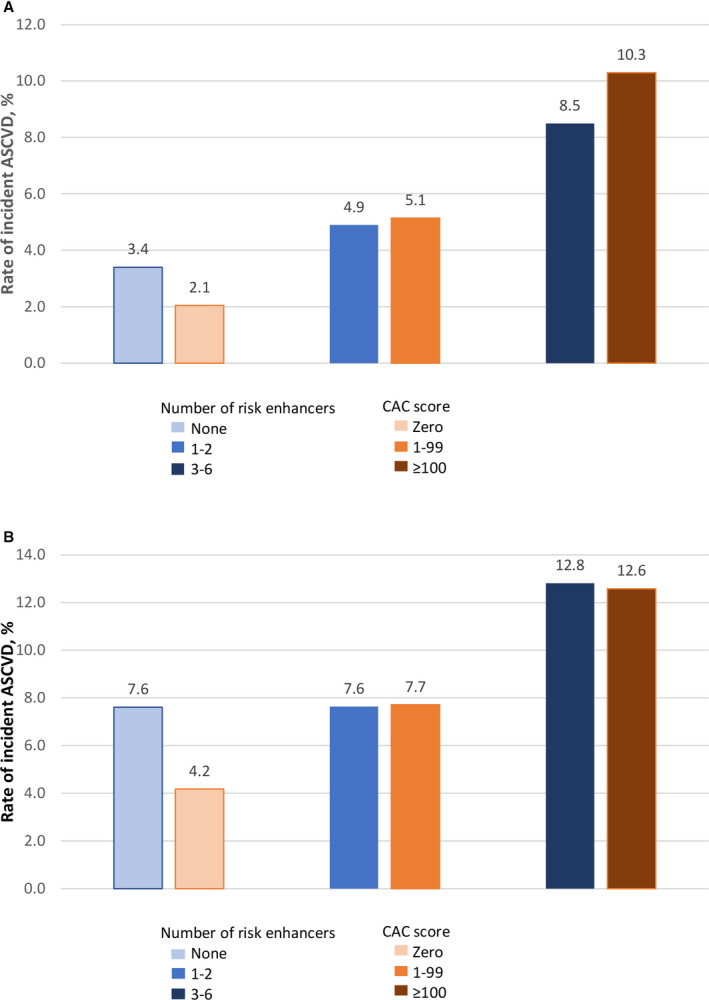
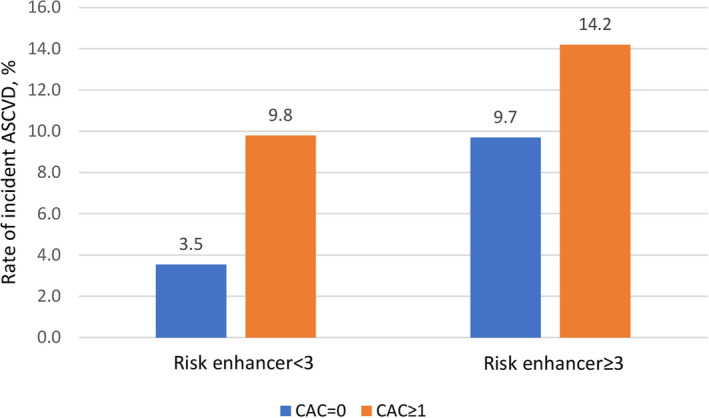
Background Limited data exist on the incremental value of the risk enhancers recommended in the 2018 American Heart Association/American College of Cardiology (ACC/AHA) cholesterol treatment guidelines in addition to the pooled cohort equation. Methods and Results Using pooled individual-level data from 3 epidemiological cohorts involving 22 942 participants (56% women, mean age 59 years), we evaluated the predictive ability of the risk enhancers and coronary artery calcium (CAC) score for atherosclerotic cardiovascular disease, and determined their incremental utility using the C statistic, net reclassification index, and integrated discrimination index. A total of 1960 (8.5%) atherosclerotic cardiovascular disease events were accrued over 10 years. Of the 10 risk enhancers evaluated, only 6 predicted atherosclerotic cardiovascular disease independent of the pooled cohort equation. However, the individual enhancers demonstrated little or no incremental benefit. There was more incremental value from combining the 6 enhancers into an aggregate score (hazard ratio [HR], 1.21; 95% CI, 1.08-1.37 for each additional enhancer), and having ≥3 enhancers represents an optimum threshold for incremental prediction (C statistic, 0.766; net reclassification index, 0.041; integrated discrimination index, 0.010; P≤0.007). On the other hand, CAC was superior to individual enhancers (C statistic, 0.774; net reclassification index, 0.073; integrated discrimination index, 0.010; P<0.001), reliably reclassifies intermediate-risk participants with <3 risk enhancers (event rate, 3.5% if no CAC and 9.8% if positive CAC), but offered no reclassification among participants with ≥3 enhancers. Conclusions The individual risk enhancers evaluated in this study provided no or only marginal incremental information added to the pooled cohort equation. However, the presence of ≥3 risk enhancers reliably identified intermediate-risk patients that will benefit from statin therapy, and further CAC testing may be considered among those with <3 risk enhancers.
Keywords: cholesterol; guidelines; pooled cohort equation; risk factors.
Conflict of interest statement
None.
Figures
References
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella‐Tommasino J, Forman DE, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation. 2019;139:e1082–e1143. DOI: 10.1161/CIR.0000000000000625. - DOI - PMC - PubMed
-
- DeFilippis AP, Young R, McEvoy JW, Michos ED, Sandfort V, Kronmal RA, McClelland RL, Blaha MJ. Risk score overestimation: the impact of individual cardiovascular risk factors and preventive therapies on the performance of the American Heart Association‐American College of Cardiology‐Atherosclerotic Cardiovascular Disease risk score in a modern multi‐ethnic cohort. Eur Heart J. 2017;38:598–608. DOI: 10.1093/eurheartj/ehw301. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
