

The feasibility and outcome of a community-based primary prevention program for cardiovascular disease in the 21st century
- PMID: 34092186
- PMCID: PMC8293959
- DOI: 10.1080/02813432.2021.1913893
The feasibility and outcome of a community-based primary prevention program for cardiovascular disease in the 21st century
Abstract
Objective: There is no evidence that systematic screening and risk factor modification in an unselected, asymptomatic population will reduce cardiovascular disease (CVD) mortality. This study aimed to evaluate the effectiveness of a primary care CVD prevention program on mortality during a 13-year follow-up.
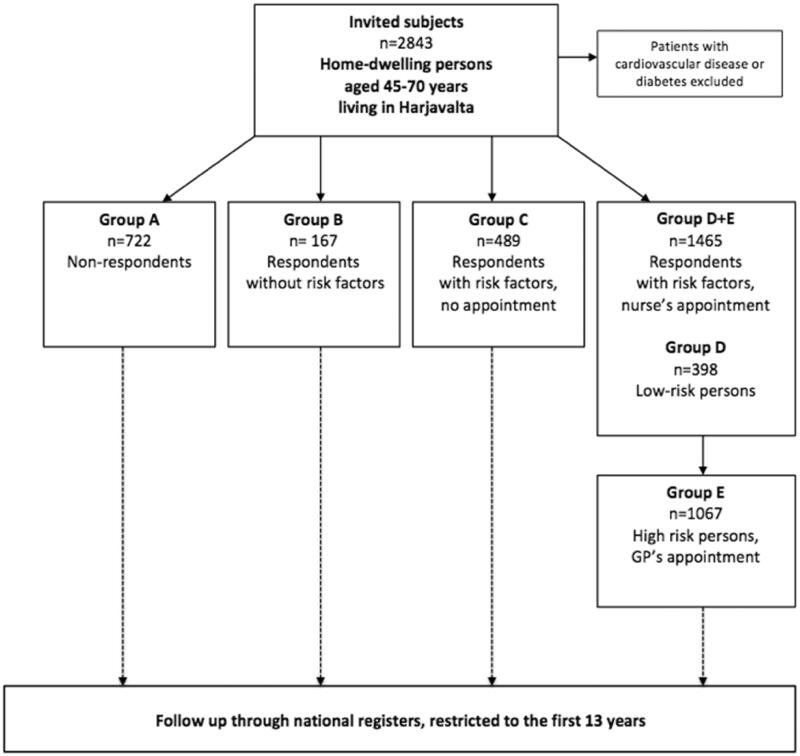
Design: A risk factor survey was sent, followed by a nurse-led lifestyle counselling to respondents with at least one CVD risk factor, and a general practitioner's (GP) appointment for high-risk persons. Screening and interventions were performed during 2005-2006.
Setting: A public health care centre in the town of Harjavalta, Finland.
Subjects: All home-dwelling 45-70-year old inhabitants without manifested CVD or diabetes.
Main outcome measures: All-cause and CVD mortality.
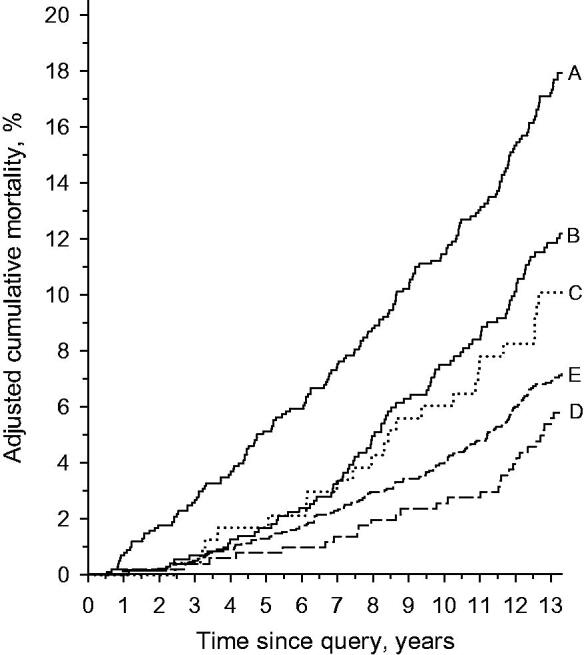
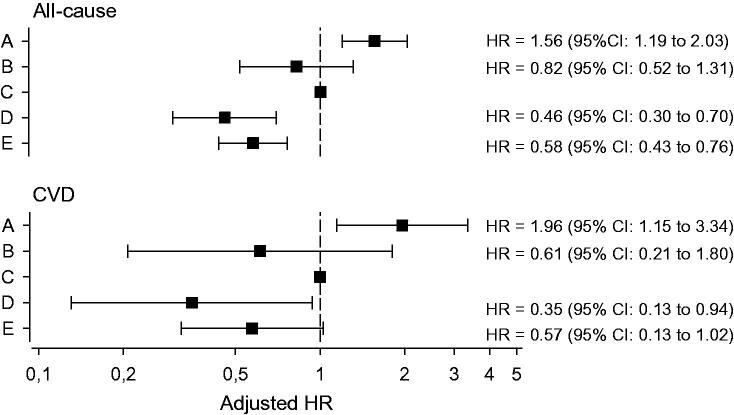
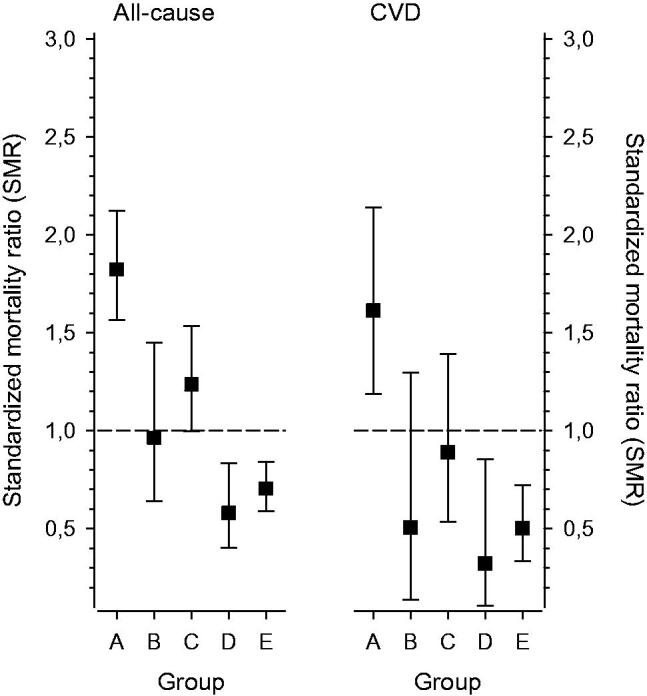
Results: Altogether 74% (2121/2856) inhabitants responded to the invitation. The intervention was received by 1465 individuals (52% of the invited population): 398 risk persons had an appointment with a nurse, followed by an appointment with a GP for 1067 high-risk persons. During the follow-up, 370 persons died. Mortality among the non-respondents was twofold compared to the participants'. In subjects who received the intervention, the age- and gender-adjusted hazard ratio for all-cause mortality was 0.44 (95% CI: 0.36 to 0.54) compared to the subjects who did not receive the intervention.
Conclusions: Reducing mortality is possible in a primary care setting by raising health awareness in the community with screening, by targeted lifestyle counselling and evidence-based preventive medication for persons at high risk for CVD. Subjects not willing to participate in health surveys have the worst prognosis.Key PointsPreviously, there is no evidence that systematic screening and risk factor modification in an unselected, asymptomatic population will reduce cardiovascular disease (CVD) mortality.With a stepwise screening program it is possible to scale the magnitude of CVD prevention in the community.Reducing mortality in a community is possible by screening, targeted lifestyle counselling, and by evidence-based preventive medication for high-risk persons.Subjects not willing to participate in health surveys have the worst prognosis.
Keywords: Cardiovascular disease; general practice; mortality; primary prevention; screening.
Conflict of interest statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Figures
Similar articles
-
Observed changes in cardiovascular risk factors among high-risk middle-aged men who received lifestyle counselling: a 5-year follow-up.Scand J Prim Health Care. 2016 Dec;34(4):336-342. doi: 10.1080/02813432.2016.1248649. Epub 2016 Nov 8. Scand J Prim Health Care. 2016. PMID: 27822969 Free PMC article.
-
Personalized prevention approach with use of a web-based cardiovascular risk assessment with tailored lifestyle follow-up in primary care practice--a pilot study.Eur J Prev Cardiol. 2016 Mar;23(5):544-51. doi: 10.1177/2047487315591441. Epub 2015 Jun 16. Eur J Prev Cardiol. 2016. PMID: 26080811 Review.
-
Primary care-based, targeted screening programme to promote sustained weight management.Scand J Prim Health Care. 2014 Mar;32(1):30-6. doi: 10.3109/02813432.2014.886493. Epub 2014 Mar 5. Scand J Prim Health Care. 2014. PMID: 24592894 Free PMC article.
-
Preventing cardiovascular disease in the 21st century: therapeutic and preventive implications of current evidence.Am J Cardiovasc Drugs. 2006;6(2):87-101. doi: 10.2165/00129784-200606020-00003. Am J Cardiovasc Drugs. 2006. PMID: 16555862 Review.
-
Nurse health and lifestyle modification versus standard care in 40 to 70 year old regional adults: study protocol of the Management to Optimise Diabetes and mEtabolic syndrome Risk reduction via Nurse-led intervention (MODERN) randomized controlled trial.BMC Health Serv Res. 2017 Dec 6;17(1):813. doi: 10.1186/s12913-017-2769-z. BMC Health Serv Res. 2017. PMID: 29212477 Free PMC article. Clinical Trial.
Cited by
-
Health screening and its association with emergency department visits and related costs among home-dwelling older adults.Scand J Prim Health Care. 2025 Mar;43(1):209-218. doi: 10.1080/02813432.2024.2423233. Epub 2024 Nov 7. Scand J Prim Health Care. 2025. PMID: 39511717 Free PMC article.
-
Are doctors using more preventive medication for cardiovascular disease? A Swedish cross-sectional study.Scand J Prim Health Care. 2023 Sep;41(3):297-305. doi: 10.1080/02813432.2023.2234439. Epub 2023 Jul 19. Scand J Prim Health Care. 2023. PMID: 37467115 Free PMC article.
-
Depressive symptoms and mortality - effect variation by body mass index: a prospective study in a primary care population.Int J Obes (Lond). 2023 Jun;47(6):512-519. doi: 10.1038/s41366-023-01296-3. Epub 2023 Mar 28. Int J Obes (Lond). 2023. PMID: 36977790 Free PMC article.
-
A real opportunity to modify cardiovascular risk through primary care and prevention: A pilot study.Front Public Health. 2023 Jan 10;10:1009246. doi: 10.3389/fpubh.2022.1009246. eCollection 2022. Front Public Health. 2023. PMID: 36703856 Free PMC article.
-
Association of unemployment and increased depressive symptoms with all-cause mortality: follow-up study of a cardiovascular prevention programme.Eur J Public Health. 2024 Dec 1;34(6):1140-1145. doi: 10.1093/eurpub/ckae175. Eur J Public Health. 2024. PMID: 39545477 Free PMC article.
References
-
- WHO . WHO fact sheet the top 10 causes of death. 2019. [Accessed 10 Sep 2019]. Available at: https://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of...
-
- Jousilahti P, Laatikainen T, Salomaa V, et al. . 40-Year CHD mortality trends and the role of risk factors in mortality decline: the North Karelia project experience. Glob Heart. 2016;11(2):207–212. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources